The clinical information regarding Understanding Raynaud's Syndrome in this article has been rigorously verified against the latest guidelines from the American College of Rheumatology (ACR) and primary research from databases like PubMed. This piece was reviewed for accuracy and patient-centric clarity and was last updated in October 2023.
Introduction
introductionRaynaud's Syndrome, often called Raynaud's Phenomenon, is a condition characterized by exaggerated vascular responses to cold temperatures or emotional stress. This response, known as a vasospasm, causes a temporary narrowing of the blood vessels, drastically reducing blood flow to the extremities. While it most commonly affects the fingers and toes, it can also impact the nose, lips, ears, and even nipples. Affecting an estimated 3-5% of the general population, it is significantly more common in women. This guide offers a comprehensive overview for those seeking to understand, manage, and treat this often-distressing condition.
What is Raynaud's Syndrome?
what-is-raynaud's-syndrome
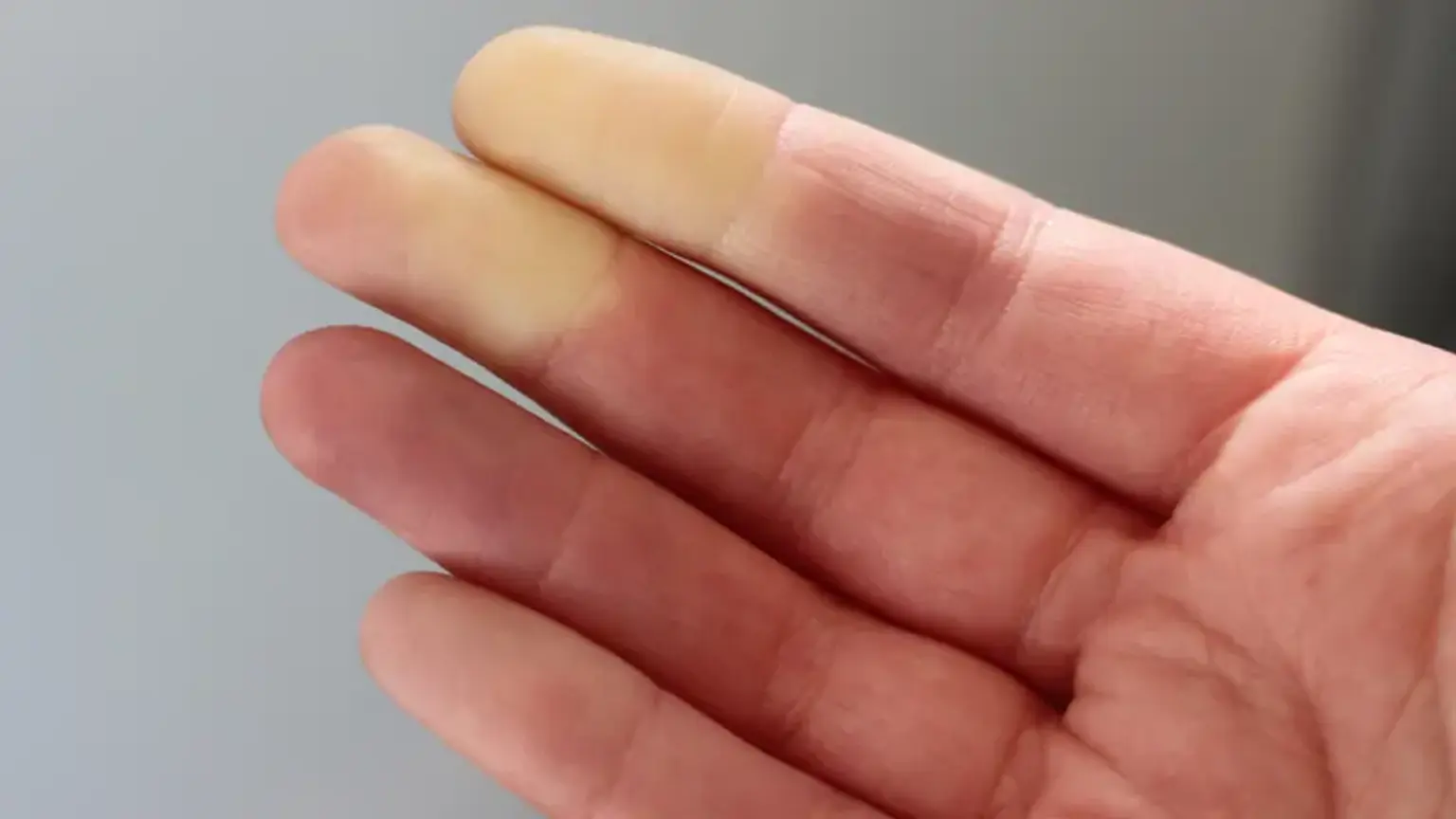
Raynaud's Syndrome is a disorder of the blood vessels. During an attack, small arteries that supply blood to the skin constrict excessively. This vasospasm limits blood circulation to affected areas, leading to a characteristic sequence of color changes in the skin. The affected skin typically turns white pallor due to the lack of blood flow, then blue cyanosis as the trapped blood loses oxygen. As the episode subsides and blood flow returns, the area often turns bright red rubor and may be accompanied by throbbing, tingling, or a painful burning sensation.
There are two main classifications of the condition, and understanding the difference is critical for proper management.
What is the Difference Between Primary and Secondary Raynaud's?
what-is-the-difference-between-primary-and-secondary-raynaud'sDistinguishing between primary and secondary Raynaud's is the most crucial step in diagnosis, as it dictates the treatment path and long-term outlook.
Primary Raynaud's
Definition: This is the most common form. It occurs on its own, without being associated with another medical condition.
Severity: Symptoms are typically milder and more of a nuisance than a cause for serious medical concern.
Complications: It rarely causes tissue damage, such as digital ulcers.
Onset: Usually begins between the ages of 15 and 30.
Secondary Raynaud's
Definition: This form is caused by an underlying problem. It is secondary to another disease, condition, or external factor.
Severity: Tends to be more complex and severe. The vasospastic attacks can be intense enough to cause painful sores or, in rare cases, tissue death gangrene.
Common Causes:
Connective Tissue Diseases: A majority of cases are linked to conditions like scleroderma systemic sclerosis, lupus, rheumatoid arthritis, and Sjogren's syndrome. About 90% of people with scleroderma experience Raynaud's.
Arterial Diseases: Conditions that damage arteries, such as atherosclerosis.
Carpal Tunnel Syndrome: Pressure on nerves in the hand can increase susceptibility.
Repetitive Action or Vibration: Typing, playing the piano, or using vibrating tools for long periods can trigger it.
Smoking: Nicotine constricts blood vessels.
Medications: Certain drugs, including beta-blockers, some migraine medications, and chemotherapy agents, can induce or worsen Raynaud's.
Onset: Typically appears later in life, usually after age 40.
What Triggers a Raynaud's Attack?
what-triggers-a-raynaud's-attackThe direct answer is that an attack is triggered by an overreaction of the blood vessels to specific stimuli. Recognizing and avoiding these triggers is the first line of defense.
Cold Temperatures: This is the most common trigger. Even minor exposures, like reaching into a freezer or being in an air-conditioned room, can initiate an attack.
Emotional Stress: Anxiety, excitement, or any strong emotional response can cause the body to release adrenaline, which constricts blood vessels and can trigger an episode.
Hormonal Changes: Fluctuations in hormones can influence the condition, which may explain why it is more prevalent in women.
Certain Medications & Substances: As mentioned, substances that constrict blood vessels, like caffeine, nicotine, and some over-the-counter cold medicines, can be potent triggers.
What are the Symptoms and Signs of Raynaud's?
what-are-the-symptoms-and-signs-of-raynaud'sWhile the color changes are the hallmark sign, individuals may experience a range of symptoms during an attack.
Distinct Color Changes: The classic progression is from white pallor, to blue cyanosis, and finally to red rubor as circulation returns.
Numbness and Cold Feeling: The affected area will feel cold to the touch and numb due to the lack of blood flow.
Sensory Changes Upon Rewarming: As blood returns, individuals often feel a painful throbbing, tingling, or a pins-and-needles sensation.
Skin Ulcers and Gangrene: In severe cases of secondary Raynaud's, prolonged or frequent attacks can lead to painful sores digital ulcers on the fingertips or toes. If left untreated, this can progress to tissue death, though this is rare.
How is Raynaud's Officially Diagnosed?
how-is-raynaud's-officially-diagnosedA definitive diagnosis requires a thorough evaluation by a healthcare provider, typically a rheumatologist. The diagnostic process focuses on identifying the symptoms and, crucially, determining if the condition is primary or secondary.
Medical History and Symptom Description: The doctor will ask detailed questions about your symptoms, triggers, and any family history of rheumatologic diseases.
Physical Examination: The doctor will examine your fingers and toes for any signs of skin changes, ulcers, or other abnormalities.
Nailfold Capillaroscopy: This is a key test to differentiate primary from secondary Raynaud's. The doctor places a drop of oil at the base of your fingernail and examines the area under a microscope. In healthy individuals or those with primary Raynaud's, the capillaries appear normal and uniform. In patients with secondary Raynaud's related to a connective tissue disease, the capillaries are often enlarged, misshapen, or reduced in number.
Blood Tests:
Antinuclear Antibody (ANA) Test: This test checks for the presence of autoantibodies, which are common in people with autoimmune diseases like lupus or scleroderma.
Erythrocyte Sedimentation Rate (ESR): This is a general inflammation marker that can be elevated in the presence of an underlying inflammatory or autoimmune condition.
What are the Best Treatments for Severe Raynaud's?
what-are-the-best-treatments-for-severe-raynaud'sTreatment goals are to reduce the frequency and severity of attacks, prevent tissue damage, and address any underlying disease.
Lifestyle & Prevention:
Dressing Warmly: Wear layers, hats, scarves, and insulated gloves or mittens.
Avoiding Cold: Use insulated drinking glasses, pre-heat your car in winter, and avoid overly aggressive air conditioning.
Stress Management: Practice relaxation techniques like mindfulness or yoga.
Quit Smoking: Eliminating nicotine is one of the most effective single steps.
Medications:
Calcium Channel Blockers: Drugs like nifedipine and amlodipine relax and open small blood vessels. They are the most common and effective prescription treatment.
Vasodilators: Medications that relax blood vessels, such as nitroglycerin cream applied to the base of the fingers, can help heal skin ulcers.
Other Medications: For severe cases, drugs like phosphodiesterase inhibitors sildenafil or antidepressants that affect serotonin levels fluoxetine may be prescribed off-label.
Medical Procedures and Surgery:
Nerve Surgery: Surgeons can cut the tiny nerves that control blood vessel constriction in the hands or feet. This can reduce the frequency and severity of attacks, but its effectiveness can wane over time.
Chemical Injections: Injections of local anesthetics or Botox can block sympathetic nerves and provide temporary relief.
IVIG Therapy or Biologic Therapy: If the Raynaud's is secondary to a severe autoimmune disease, treating the underlying condition with powerful immunomodulating drugs is the primary strategy.
How Can I Manage Living with Raynaud's?
how-can-i-manage-living-with-raynaud's"For years, every winter was a nightmare of painful, white fingers that felt completely dead. Getting a clear diagnosis and learning the right management techniques, like using heated gloves and avoiding sudden cold, gave me back control over my life and a sense of security." – An anonymous patient, Canada.
Living with Raynaud's is about proactive management. This includes carrying an emergency kit with gloves and hand warmers, using apps to check weather forecasts, and educating friends and family about the condition to avoid misunderstandings about your need for warmth.
When Should I See a Doctor for Raynaud's?
when-should-i-see-a-doctor-for-raynaud'sYou should consult a doctor if you experience symptoms of Raynaud's. It is especially urgent to seek medical evaluation if you notice any of the following, as they may indicate a more serious underlying secondary condition:
Symptoms appear after age 30.
The attacks are very severe or getting worse.
You develop a sore or ulcer on a finger or toe.
Symptoms are only on one side of your body.
You have other symptoms like joint pain, skin rashes, skin thickening, or significant fatigue.
Recommended Clinics with Relevant Expertise in South Korea
recommended-clinics-with-relevant-expertise-in-south-koreaFor individuals seeking evaluation for Raynaud's and related rheumatologic conditions, South Korea offers numerous world-class medical centers with comprehensive diagnostic and treatment capabilities.
Website | Clinic Name | Best Known For | Address | Contact |
|---|---|---|---|---|
Cha University Bundang Medical Center | Comprehensive care across all medical specialties | Bundang-gu, Gyeonggi-do, South Korea | ||
Seoul St. Mary's Hospital-Seocho | Advanced research and treatment in autoimmune diseases | Seocho-gu, Seoul, South Korea | ||
Design Hospital | Specialized surgical and advanced medical care | Deokjin-gu, Jeollabuk-do, South Korea | ||
Kyungpook National University Chilgok Hospital | Leading research in geriatric and chronic diseases | Buk-gu, Daegu, South Korea | ||
Wooridul Hospital Gangnam | Spine and joint specialty, potential overlap with rheumatic pain | Gangnam-gu, Seoul, South Korea | ||
Nanoori Hospital, Gangnam | Renowned spine and joint treatment center | Gangnam-gu, Seoul, South Korea | ||
Mokdong Hospital Ewha Womans University | Strong focus on women's health and research medicine | Yangcheon-gu, Seoul, South Korea | ||
Sarang Plus Hospital | Comprehensive general and specialized medical services | Gangdong-gu, Seoul, South Korea |
Recommended Treatment/Procedure Names with Average Costs in South Korea
recommended-treatmentprocedure-names-with-average-costs-in-south-koreaTreatment for Raynaud's itself is often lifestyle-based or pharmacological. However, for secondary Raynaud's, managing the underlying rheumatologic condition is key. Below are costs for common rheumatology treatments in South Korea.
Treatment/Procedure Name | Treatment Duration | Hospitalization? | Avg Cost Range (USD) in S. Korea | Contact |
|---|---|---|---|---|
Biologic Therapy for Rheumatoid Arthritis | 1-4 hours | Not Needed | $1,500 - $4,000 | |
Stem Cell Therapy for Autoimmune Diseases | 1-2 hours | Not Needed | $15,000 - $30,000 | |
Immunosuppressive Therapy | 2-3 hours | Not Needed | $500 - $2,500 | |
IVIG Therapy (Intravenous Immunoglobulin) | 3-6 hours | Not Needed | $2,000 - $7,000 | |
Targeted DMARDs | 1-2 hours | Not Needed | $1,000 - $5,000 | |
Lupus Nephritis Management | 2-4 hours | Not Needed | $10,000 - $25,000 | |
Vasculitis Treatment | 1-2 hours | Not Needed | $8,000 - $20,000 | |
Systemic Sclerosis Treatment | 1-3 hours | Not Needed | $1,000 - $2,000 |
What Are Common Questions About Raynaud's Syndrome?
what-are-common-questions-about-raynaud's-syndromeThis section addresses practical questions patients often have.
1. Is Raynaud's hereditary?
1.-is-raynaud's-hereditaryThere appears to be a genetic component. Having a first-degree relative parent, sibling, or child with primary Raynaud's disease increases your risk of developing the condition.
2. Can diet affect my Raynaud's symptoms?
2.-can-diet-affect-my-raynaud's-symptomsWhile no specific diet cures Raynaud's, some dietary choices can help. Consuming omega-3 fatty acids found in fish oil and ginkgo biloba may help improve circulation for some individuals, but you must consult a doctor before starting any supplements. Avoiding caffeine, which is a vasoconstrictor, can also be beneficial.
3. Can Raynaud's be permanently cured?
3.-can-raynaud's-be-permanently-curedPrimary Raynaud's cannot be cured, but it can be managed effectively with lifestyle changes and does not typically worsen over time. Secondary Raynaud's also cannot be cured, and its management is tied directly to treating the underlying disease. Effective management of the primary condition can significantly reduce the severity of Raynaud's symptoms.
4. Does Raynaud's affect other parts of the body besides fingers and toes?
4.-does-raynaud's-affect-other-parts-of-the-body-besides-fingers-and-toesYes. While less common, Raynaud's attacks can affect the nose, lips, ears, and even nipples. The mechanism of vasospasm is the same regardless of the location.
5. Is Raynaud's Syndrome an autoimmune disease?
5.-is-raynaud's-syndrome-an-autoimmune-diseasePrimary Raynaud's is not an autoimmune disease; it is a vascular disorder. However, secondary Raynaud's is very frequently a symptom of an underlying autoimmune disease, such as lupus, scleroderma, or rheumatoid arthritis. This is why a thorough diagnostic workup is essential.
Take Control of Your Symptoms: Find Your Raynaud's Treatment Path
take-control-of-your-symptoms:-find-your-raynaud's-treatment-pathUnderstanding the source of your symptoms is the first and most critical step toward effective management. Whether you are seeking a definitive diagnosis or exploring advanced treatment for an underlying condition, a clear path forward is available. We encourage you to take the next step. By inquiring through our service, you gain access to a seamless, transparent process and a dedicated Care Manager who provides end-to-end support, from initial questions to post-recovery care. And Start Your Confidential Inquiry With CloudHospital.