The clinical information regarding Diverticulitis in this article has been rigorously verified against the latest clinical practice updates from the American Gastroenterological Association (AGA) and primary research from databases like PubMed. This piece was reviewed for accuracy and patient-centric clarity and was last updated in August 2021.
Introduction
introductionDiverticulitis is a common digestive condition that can cause significant discomfort and, in some cases, lead to serious complications. It occurs when small, bulging pouches that can form in the lining of your digestive system known as diverticula become inflamed or infected. While the presence of these pouches diverticulosis is very common, especially after age 40, active diverticulitis affects a smaller but significant portion of individuals. This guide offers a comprehensive overview of diverticulitis for those seeking to understand its causes, recognize its symptoms, and explore effective management and treatment options.
What is Diverticulitis?
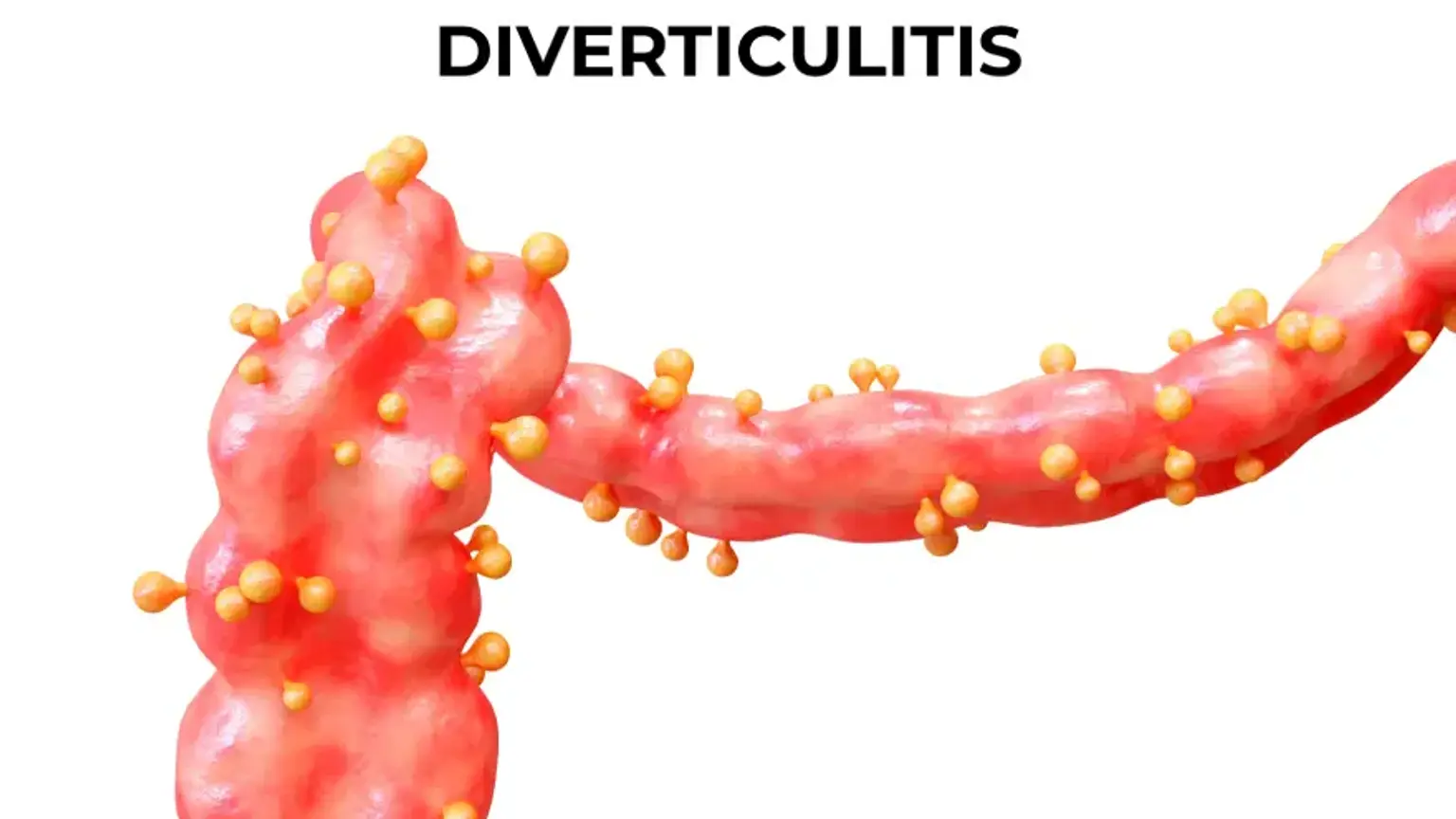
what-is-diverticulitisTo understand diverticulitis, it is essential first to understand diverticulosis. Diverticulosis refers to the presence of small pouches, or diverticula, that develop in the wall of the colon, most commonly in the lower part known as the sigmoid colon. These pouches form in naturally weak spots in the colon wall under pressure. For many people, diverticulosis causes no symptoms.
Diverticulitis occurs when one or more of these pouches become inflamed or infected. This can happen when stool or bacteria get trapped in a pouch, leading to symptoms that range from mild abdominal pain to severe infection and complications like an abscess or a tear perforation in the colon wall.
What is the Main Cause of Diverticulitis?
what-is-the-main-cause-of-diverticulitisThe main cause of diverticulitis is the inflammation or infection of pre existing diverticula in the colon wall. While the exact trigger for this inflammation is not always clear, it is strongly linked to a combination of anatomical factors and lifestyle influences. The prevailing theory for decades has been that a low fiber diet is a primary risk factor. A lack of dietary fiber can lead to constipation and increased pressure inside the colon, which may contribute to both the formation of diverticula and the risk of them becoming inflamed.
Other significant risk factors include:
Age: The risk increases significantly after the age of 40.
Obesity: Being severely overweight increases the likelihood of developing diverticulitis.
Smoking: Smokers are at a higher risk compared to non-smokers.
Lack of Exercise: Vigorous physical activity appears to be protective against diverticulitis.
Certain Medications: Some drugs, including steroids, opioids, and nonsteroidal anti-inflammatory drugs like ibuprofen, are associated with an increased risk.
What are the First Symptoms of Diverticulitis?
what-are-the-first-symptoms-of-diverticulitisThe first and most common symptom of diverticulitis is a persistent and often severe pain in the lower left abdomen. This is the most frequent location because the sigmoid colon is the most common site for diverticula. However, the pain can also occur in the right side of the abdomen, particularly in individuals of Asian descent.
Beyond abdominal pain, initial signs and symptoms of a diverticulitis flare up often include:
Fever and chills
Nausea and sometimes vomiting
Abdominal tenderness, especially upon touch
A change in bowel habits, such as constipation or, less commonly, diarrhea
Bloating and gas
How is Diverticulitis Officially Diagnosed?
how-is-diverticulitis-officially-diagnosedDiverticulitis is officially diagnosed through a combination of a medical history review, a physical examination, and diagnostic imaging tests. During the physical exam, a doctor will check your abdomen for tenderness. To confirm the diagnosis and rule out other conditions with similar symptoms such as appendicitis or an ovarian cyst, one or more tests are typically ordered.
The diagnostic process usually involves:
Blood and Urine Tests: These can identify signs of infection, such as an elevated white blood cell count.
CT (Computed Tomography) Scan: This is the most common and accurate imaging test used to diagnose acute diverticulitis. It can clearly show the inflamed pouches and reveal the severity of the condition, including the presence of any complications like an abscess or perforation.
Colonoscopy: A colonoscopy is generally not performed during an acute diverticulitis attack due to the risk of perforating the inflamed colon. However, a doctor will typically recommend one about six to eight weeks after recovery to examine the full colon and rule out other conditions, such as colorectal cancer.
What are the Treatment Options for Diverticulitis?
what-are-the-treatment-options-for-diverticulitisTreatment for diverticulitis depends entirely on the severity of your symptoms and whether you have any complications.
Uncomplicated Diverticulitis
uncomplicated-diverticulitisFor mild cases, treatment can often be managed at home and typically involves:
Dietary Changes: Your doctor may recommend a clear liquid diet for a few days to allow your colon to heal. As symptoms improve, you will gradually reintroduce low fiber foods, eventually progressing to a high fiber diet to help prevent future flare ups.
Antibiotics: Oral antibiotics are often prescribed to treat the infection, though recent guidelines suggest they may not be necessary in very mild cases.
Complicated Diverticulitis
complicated-diverticulitisFor severe symptoms or the presence of complications, hospitalization is necessary. Treatment may include:
Intravenous (IV) Antibiotics: Delivering antibiotics directly into the bloodstream works faster and more effectively for serious infections.
Abscess Drainage: If a pus filled pocket abscess has formed, it may need to be drained. This is often done percutaneously, where a radiologist inserts a needle through the skin to drain the fluid, guided by a CT scan.
Surgical Intervention: Surgery becomes necessary for serious complications or recurrent, severe attacks.
When Does Diverticulitis Require Surgery?
when-does-diverticulitis-require-surgerySurgery for diverticulitis is required when complications arise that cannot be managed with conservative treatments or when a patient suffers from frequent, severe flare ups that impact their quality of life. The primary surgical procedure performed is a colectomy, which involves removing the diseased segment of the colon.
Specific indications for surgery include:
A perforation in the colon wall, leading to peritonitis, a life threatening infection of the abdominal lining.
An abscess that is too large to be drained with a needle or does not respond to drainage.
A fistula, which is an abnormal passageway that forms between the colon and another organ, such as the bladder or vagina.
A bowel obstruction or stricture narrowing in the colon caused by repeated scarring.
Multiple, severe episodes of uncomplicated diverticulitis that do not respond well to medical management.
"The pain came on so suddenly and was so intense, I was sure it was something terrible. Getting the diverticulitis diagnosis was actually a relief. Learning to manage my diet has given me control back over my life." – an anonymous patient, United Kingdom.
When Should I See a Doctor for Diverticulitis?
when-should-i-see-a-doctor-for-diverticulitisYou should seek medical attention promptly if you experience the hallmark symptoms of diverticulitis, especially for the first time. Early diagnosis and treatment can help prevent serious complications.
Contact your doctor immediately if you experience:
Severe, persistent abdominal pain, particularly in the lower left side.
Unexplained fever accompanied by abdominal pain.
Inability to tolerate liquids or food.
Persistent nausea and vomiting.
Noticeable bleeding from your rectum.
Recommended Clinics with Relevant Expertise in South Korea
recommended-clinics-with-relevant-expertise-in-south-koreaSouth Korea is home to world-class medical centers with advanced gastroenterology departments specializing in the diagnosis and treatment of digestive diseases like diverticulitis.
Website | Clinic Name | Best Known For | Address | Contact |
|---|---|---|---|---|
Asan Medical Center | Comprehensive Digestive Disease Center & Research | Songpa-gu, Seoul,South Korea | ||
Seoul St. Mary's Hospital-Seocho | Advanced Endoscopic Procedures & IBD Care | Seocho-gu, Seoul,South Korea | ||
Seoul National University Hospital- gangnam district | Leading Surgical Gastroenterology & Cancer Treatment | Gangnam-gu, Seoul, South Korea | ||
Kangdong Sacred Heart Hospital | Minimally Invasive Colorectal Surgery | Gangdong-gu, Seoul, South Korea | ||
H Plus Yangji Hospital | Specialized Digestive Endoscopy Center | Gwanak-gu, Seoul, South Korea | ||
Soon Chun Hyang University Hospital Seoul | High-Volume Gastroenterology & Hepatology Services | Yongsan-gu, Seoul, South Korea | ||
Kyung Hee University Hospital At Gangdong | Integrative Medicine & Digestive Health | Gangdong-gu, Seoul, South Korea | ||
Hanyang University Seoul Hospital | Expertise in Complex Gastrointestinal Disorders | Seongdong-gu, Seoul,South Korea |
Recommended Treatment/Procedure Names with Average Costs in South Korea
recommended-treatmentprocedure-names-with-average-costs-in-south-koreaThe following table outlines common diagnostic and therapeutic procedures related to gastroenterology, including those for diverticulitis, with estimated data for South Korea.
Treatment/Procedure Name | Treatment Duration | Hospitalization? | Avg Cost Range (USD) in S. Korea | Contact |
|---|---|---|---|---|
Colonoscopy with Polypectomy | 30-60 mins | Not Needed | $800 - $1,500 | |
Colon Cancer Surgery (Colectomy) | 2-4 hours | Needed (3-7 days) | $15,000 - $25,000 | |
Upper GI Endoscopy with Biopsy (EGD) | 15-30 mins | Not Needed | $600 - $1,200 | |
ERCP with Stenting | 30-90 mins | Needed (overnight) | $3,000 - $6,000 | |
Endoscopic Ultrasound (EUS) with Aspiration | 30-60 mins | Not Needed | $1,500 - $3,000 | |
Bariatric Surgery (Gastric Bypass) | 2-4 hours | Needed (2-3 days) | $14,000 - $22,000 | |
IBD Biologic Therapy | 30 mins - 2 hours | Not Needed | $2,000 - $5,000 | |
Pancreatic Surgery (Whipple Procedure) | 4-8 hours | Needed (7-14 days) | $45,000 - $70,000 | |
Hepatitis C Antiviral Therapy | 8 to 12 weeks | Not Needed | $20,000 - $40,000 | |
Liver Transplantation | 6-12 hours | Needed | $120,000 - $180,000 |
What Are Common Questions About Diverticulitis?
what-are-common-questions-about-diverticulitisThis section addresses the most common practical questions patients have about living with the condition.
1. What foods should you avoid during a diverticulitis flare-up?
1.-what-foods-should-you-avoid-during-a-diverticulitis-flare-upDuring an acute flare up, you must avoid high-fiber foods to let your colon rest. Your doctor will likely recommend a clear liquid diet broth, clear juices, water for a few days. As you recover, you will move to low-fiber foods like white bread, white rice, and eggs before gradually reintroducing fiber. The old advice to avoid nuts, seeds, and popcorn is now considered outdated for most people.
2. Can diverticulitis be completely cured?
2.-can-diverticulitis-be-completely-curedDiverticulitis itself, as an episode of inflammation, can be cured with treatment. However, the underlying condition of diverticulosis the presence of the pouches is permanent. The goal of long-term management is to prevent future flare-ups of diverticulitis through diet and lifestyle changes. Surgery to remove the affected part of the colon is the closest thing to a cure for recurrent disease in that specific segment.
3. How long does a diverticulitis flare-up last?
3.-how-long-does-a-diverticulitis-flare-up-lastThe duration of a flare up varies by its severity. For uncomplicated cases treated at home with antibiotics and a liquid diet, patients often start to feel better within two to three days. A full recovery can take about a week. For complicated cases requiring hospitalization, recovery will take longer, depending on the specific treatments needed.
4. Is diverticulitis related to colorectal cancer?
4.-is-diverticulitis-related-to-colorectal-cancerDiverticulitis is not a direct cause of colorectal cancer, and having it does not increase your risk of developing cancer. However, the symptoms of diverticulitis can sometimes mimic those of colorectal cancer. This is why a follow up colonoscopy after an acute attack is critical to rule out cancer or other serious conditions.
Tired of Pain and Uncertainty: Get a Personalized Diverticulitis Action Plan Now
tired-of-pain-and-uncertainty-get-a-personalized-diverticulitis-action-planNavigating a diverticulitis diagnosis is stressful, but you're not alone. World-class specialists in South Korea offer advanced diagnostics and a full spectrum of treatments, from dietary management to minimally invasive surgery. We provide a seamless, transparent process guided by a dedicated Care Manager for support from start to finish. Take the first step toward lasting relief and Start Your Confidential Inquiry with CloudHospital.