The clinical information regarding Anemia of Chronic Disease in this article has been rigorously verified against the latest guidelines from the American Society of Hematology (ASH) and primary research from databases like PubMed. This piece was reviewed for accuracy and patient-centric clarity and was last updated in March 2023.
Introduction
introductionAnemia of Chronic Disease (ACD), also known as anemia of inflammation, is the second most common type of anemia worldwide, after iron deficiency anemia. It is not a disease in itself but a complication arising from a persistent, underlying inflammatory, infectious, or malignant condition. For patients managing a chronic illness, the development of ACD can significantly impact quality of life, increasing fatigue and decreasing physical function. This guide provides a comprehensive overview of ACD, from its fundamental causes to the most advanced treatment strategies.
What is Anemia of Chronic Disease?
what-is-anemia-of-chronic-disease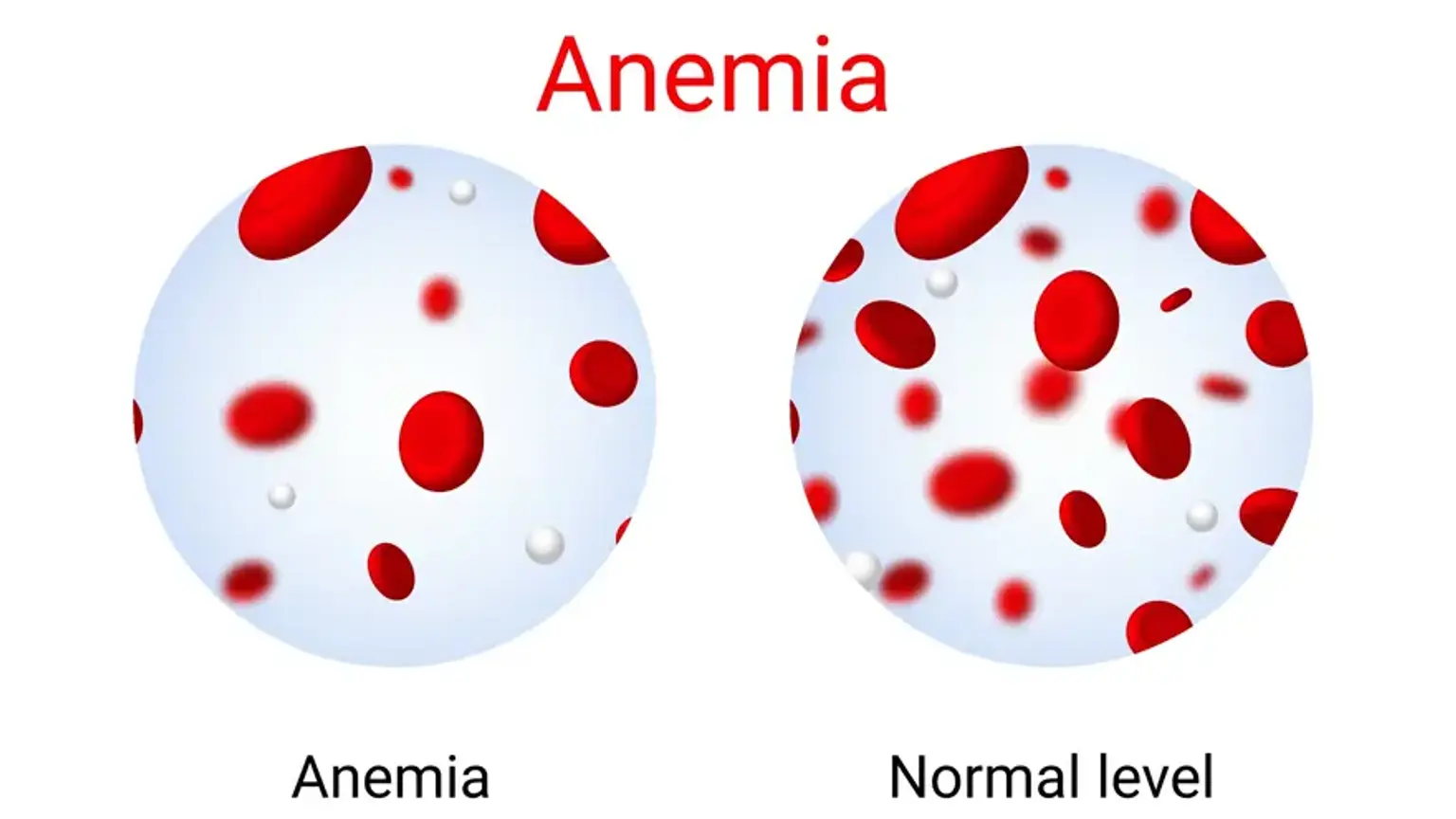
Anemia of Chronic Disease is a type of anemia that develops in patients with long standing medical conditions involving inflammation. In a healthy state, the body maintains a precise balance of red blood cell production, a process called erythropoiesis. During chronic inflammation, the body's immune response disrupts this balance through several key mechanisms.
The central regulator in this process is a hormone called hepcidin. Produced by the liver, hepcidin levels rise dramatically in response to inflammatory signals, particularly a cytokine known as Interleukin-6. Elevated hepcidin orchestrates the development of anemia by:
Blocking Iron Absorption: It prevents the absorption of iron from the gut.
Trapping Iron in Storage: It traps iron inside storage cells like macrophages and liver cells, preventing its release into the bloodstream where it is needed to make hemoglobin for new red blood cells.
This creates a state of functional iron deficiency. Even if the body has adequate iron stores, hepcidin makes that iron unavailable for red blood cell production. Concurrently, the same inflammatory cytokines can suppress the production of Erythropoietin (EPO), a hormone made by the kidneys that signals the bone marrow to produce red blood cells and make the bone marrow less responsive to the EPO that is available.
What is the Main Cause of Anemia in Chronic Disease?
what-is-the-main-cause-of-anemia-of-chronic-diseaseThe main cause of Anemia in Chronic Disease is sustained systemic inflammation from an underlying condition. The body's immune response to these conditions triggers the release of cytokines that alter iron metabolism and red blood cell production. The conditions are broadly grouped into three categories:
Chronic Inflammatory Diseases: These are the most common causes. Examples include rheumatoid arthritis, inflammatory bowel disease Crohn's disease, ulcerative colitis, lupus, and sarcoidosis. The persistent autoimmune activity fuels the inflammatory state.
Chronic Infections: Long-term infections can lead to ACD. This includes conditions like tuberculosis (TB), HIV/AIDS, osteomyelitis bone infection, and chronic fungal infections.
Malignancy (Cancer): Many types of cancer, including lymphomas, multiple myeloma, and solid tumors like lung and breast cancer, induce a chronic inflammatory response that causes ACD. Cancer treatments like chemotherapy can also suppress bone marrow function, worsening the anemia.
Chronic Kidney Disease (CKD): While CKD involves inflammation, the primary cause of anemia in this condition is decreased production of the hormone erythropoietin (EPO) by the damaged kidneys. This is often considered a distinct but related entity.
What Are the Symptoms and Signs of ACD?
what-are-the-symptoms-and-signs-of-acdThe symptoms of Anemia of Chronic Disease are often mild to moderate and can be easily mistaken for symptoms of the underlying primary illness. This overlap can delay diagnosis.
Key signs include:
Persistent fatigue and lack of energy
Shortness of breath, especially with exertion
Pale skin
Dizziness or lightheadedness
Rapid heartbeat
Difficulty concentrating or brain fog
Feeling cold, especially in the hands and feet
How is Anemia of Chronic Disease Diagnosed?
how-is-anemia-of-chronic-disease-diagnosedDiagnosing ACD requires a careful clinical evaluation and specific laboratory tests to differentiate it from other types of anemia, particularly true iron deficiency anemia (IDA), which can also co-exist.
Initial Consultation & Physical Exam: A physician will review the patient's medical history, focusing on known chronic conditions, and perform a physical exam to check for signs like pallor.
Complete Blood Count (CBC): This is the first step. In ACD, the anemia is typically normocytic and normochromic, meaning the red blood cells are of normal size and color. In long standing cases, it can become microcytic smaller cells, mimicking IDA.
Iron Studies: This panel is critical for diagnosis.
Serum Iron: Usually low.
Total Iron-Binding Capacity (TIBC): Low or normal. This is a key differentiator, as TIBC is high in true iron deficiency.
Transferrin Saturation (TSAT): Low or normal.
Serum Ferritin: Normal or high. Ferritin is an acute phase reactant, meaning it increases with inflammation. This is the most important marker to distinguish ACD high/normal ferritin from IDA low ferritin.
Inflammatory Markers: Tests like C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are often elevated, confirming the presence of underlying inflammation.
How is Anemia in Chronic Disease Different from Iron Deficiency Anemia?
how-is-anemia-of-chronic-disease-different-from-iron-deficiency-anemiaDistinguishing between ACD and Iron Deficiency Anemia (IDA) is the central diagnostic challenge, as both can present with low serum iron. The key difference lies in the body's total iron stores, reflected by serum ferritin.
Feature | Anemia of Chronic Disease (ACD) | Iron Deficiency Anemia (IDA) |
|---|---|---|
Primary Problem | Iron is available but trapped in storage (functional deficiency) | Total body iron stores are depleted |
Serum Ferritin | Normal or High | Low |
TIBC | Low or Normal | High |
Red Blood Cell Size | Normocytic (Normal), can become microcytic | Microcytic (Small) |
Underlying Cause | Chronic inflammation, infection, or cancer | Blood loss, poor diet, malabsorption |
In some cases, a patient may have both conditions simultaneously ACD + IDA, which can complicate the diagnosis. This is common in patients with inflammatory bowel disease, where both inflammation and blood loss occur.
What Are the Most Effective Treatments for Anemia of Chronic Disease?
what-are-the-most-effective-treatments-for-anemia-of-chronic-diseaseTreatment for ACD is multi-faceted and focuses first on the underlying cause. Simply adding iron is often ineffective and can even be harmful in some infections.
1. Treat the Underlying Condition: This is the most important step. Effectively managing the primary disease e.g., controlling inflammation in rheumatoid arthritis with medication, treating a chronic infection can reduce hepcidin levels, release stored iron, and resolve the anemia on its own.
2. Erythropoiesis-Stimulating Agents (ESAs): For patients with significant, symptomatic anemia, particularly those with cancer or chronic kidney disease, ESAs are a primary treatment. These are synthetic versions of the hormone EPO e.g., epoetin alfa, darbepoetin alfa that stimulate the bone marrow to produce more red blood cells. Response rates in cancer patients are around 60%. ESAs are often given with intravenous iron to ensure the bone marrow has the necessary building blocks.
3. Iron Supplementation: Oral iron is generally not effective in ACD because hepcidin blocks its absorption. Intravenous (IV) iron can be used to bypass this block, especially when given with ESAs or if a true iron deficiency co-exists.
4. Blood Transfusions: Red blood cell transfusions are reserved for patients with severe, life threatening, or highly symptomatic anemia who require rapid correction of their hemoglobin levels. Transfusions provide immediate relief but are a temporary solution and carry risks such as infections, allergic reactions, and iron overload.
5. Emerging Therapies: Research is heavily focused on targeting the hepcidin pathway directly. Drugs that inhibit hepcidin production or activity are in clinical trials and represent a promising future for treating ACD more effectively.
"For years, the bone deep exhaustion was worse than the joint pain from my arthritis. I thought it was just part of the disease. Getting the anemia diagnosis was a turning point. The combination of better arthritis control and targeted treatment gave me back an energy I thought I’d lost forever." – An anonymous patient, United Kingdom.
When Should I See a Hematologist for Persistent Anemia?
when-should-i-see-a-hematologist-for-persistent-anemiaYou should see a doctor if you experience persistent symptoms of anemia like fatigue, shortness of breath, or dizziness. Your primary care physician can perform initial tests. A referral to a hematologist a specialist in blood disorders is recommended if:
The cause of the anemia is not clear after initial testing.
The anemia is severe or not responding to standard treatments.
You have a complex underlying condition like cancer or kidney disease requiring specialized anemia management.
There is a suspicion of a co-existing blood disorder.
Recommended Clinics with Relevant Expertise in South Korea
recommended-clinics-with-relevant-expertise-in-south-koreaSouth Korea is home to world-class medical centers with advanced haematology-oncology departments capable of diagnosing and managing complex conditions like Anemia of Chronic Disease.
Website | Clinic Name | Best Known For | Address | Contact |
|---|---|---|---|---|
Asan Medical Center | Oncology, Organ Transplantation, Cardiology | Songpa-gu, Seoul, South Korea | ||
Seoul St. Mary's Hospital | Hematology (BMT), Oncology, Organ Transplantation | Jongno-gu, Seoul, South Korea | ||
Severance Hospital | Cancer Center, Robotics Surgery, Cardiovascular | Seodaemun-gu, Seoul, South Korea | ||
Seoul Miz Hospital | Gynecology, Infertility, Pediatrics | Gangdong-gu, Seoul, South Korea | ||
Ewha Womans University Medical Center | Cancer Center, Cardiovascular, Joint/Spine | Seodaemun-gu, Seoul, South Korea | ||
G Sam Hospital | Comprehensive Care, Emergency Medicine | Gwangmyeong-si, Gyeonggi-do, South Korea | ||
Soon Chun Hyang University Bucheon Hospital | Comprehensive Care, Cancer Center | Bucheon-si, Gyeonggi-do, South Korea | ||
Kyung Hee University Hospital At Gangdong | East-West Medicine Integration, Cancer Center | Gangdong-gu, Seoul, South Korea |
Recommended Treatment/Procedure Names with Average Costs in South Korea
recommended-treatmentprocedure-names-with-average-costs-in-south-koreaThe treatments for ACD are often part of a broader strategy to manage a primary condition. The following table outlines advanced haematology-oncology procedures and supportive care options with estimated costs in South Korea. These are general estimates and can vary significantly.
Treatment/Procedure Name | Duration | Hospitalization? | Avg. Cost (USD) in S.Korea | Contact |
|---|---|---|---|---|
CAR T-cell Therapy | 40-60 days | Needed (2-4 weeks) | $370,000 - $450,000 | |
Gene Therapy | 1–5 days | Needed (1-5 days) | $2,000,000 | |
Stem Cell/Bone Marrow Transplant | 30-100 days | Needed (4-6 weeks) | $60,000 - $150,000 | |
Targeted Therapy | 3 to 12 months | Not Needed | $3,000 - $10,000 | |
Immunotherapy | 6 months | Not Needed | $5,000 - $15,000 | |
Combination Chemotherapy | 3 to 6 months | Needed (3-7 days) | $10,000 - $50,000 | |
Radiation Therapy | 2-8 weeks | Not Needed | $15,000 - $40,000 |
What Are Common Questions About Anemia of Chronic Disease?
what-are-common-questions-about-anemia-of-chronic-disease1. Can anemia of chronic disease be cured or reversed?
1.-can-anemia-of-chronic-disease-be-cured-or-reversedYes, it can often be reversed or completely resolved if the underlying chronic condition that is causing it can be effectively treated and controlled. The primary goal is always to manage the root cause of the inflammation.
2. How does hepcidin cause anemia of chronic disease?
2.-how-does-hepcidin-cause-anemia-of-chronic-diseaseHepcidin is the master regulator. It causes ACD by 1- blocking iron absorption from the diet in the intestines and 2- locking existing iron away in storage cells macrophages, making it unavailable for the bone marrow to use for producing new red blood cells.
3. Can diet and lifestyle changes help manage ACD?
3.-can-diet-and-lifestyle-changes-help-manage-acdWhile a healthy diet rich in vitamins is important for overall health, dietary changes alone cannot overcome the iron blockade caused by hepcidin in ACD. Unlike iron deficiency anemia, simply eating more iron rich foods will not resolve the issue. The focus must be on treating the primary disease.
4. What are the long-term effects of untreated anemia of chronic disease?
4.-what-are-the-long-term-effects-of-untreated-anemia-of-chronic-diseaseUntreated, persistent ACD can significantly decrease quality of life due to chronic fatigue and reduced physical capacity. In patients with cardiovascular disease, even mild anemia can worsen conditions like heart failure and increase mortality risk. It can also impair cognitive function and weaken the immune system further.
5. Is anemia of chronic disease common?
5.-is-anemia-of-chronic-disease-commonYes, it is extremely common. It is the most frequent type of anemia found in hospitalized patients and the second most common type overall. Its prevalence directly correlates with the prevalence of chronic diseases like rheumatoid arthritis, cancer, and chronic kidney disease.
Take the First Step Toward Managing Your Health Now!
take-the-first-step-toward-managing-your-healthStruggling with anemia or a chronic condition? South Korea’s top hematology-oncology centers offer expert diagnosis and treatment. Through CloudHospital Start Your Confidential Inquiry and you'll get a personalized care plan and end-to-end support from a dedicated Care Manager.