
The clinical information regarding Congenital Adrenal Hyperplasia in this article has been rigorously verified against the latest guidelines from The Endocrine Society and primary research from databases like PubMed. This piece was reviewed for accuracy and patient-centric clarity and was last updated in November 2018.
Introduction
introduction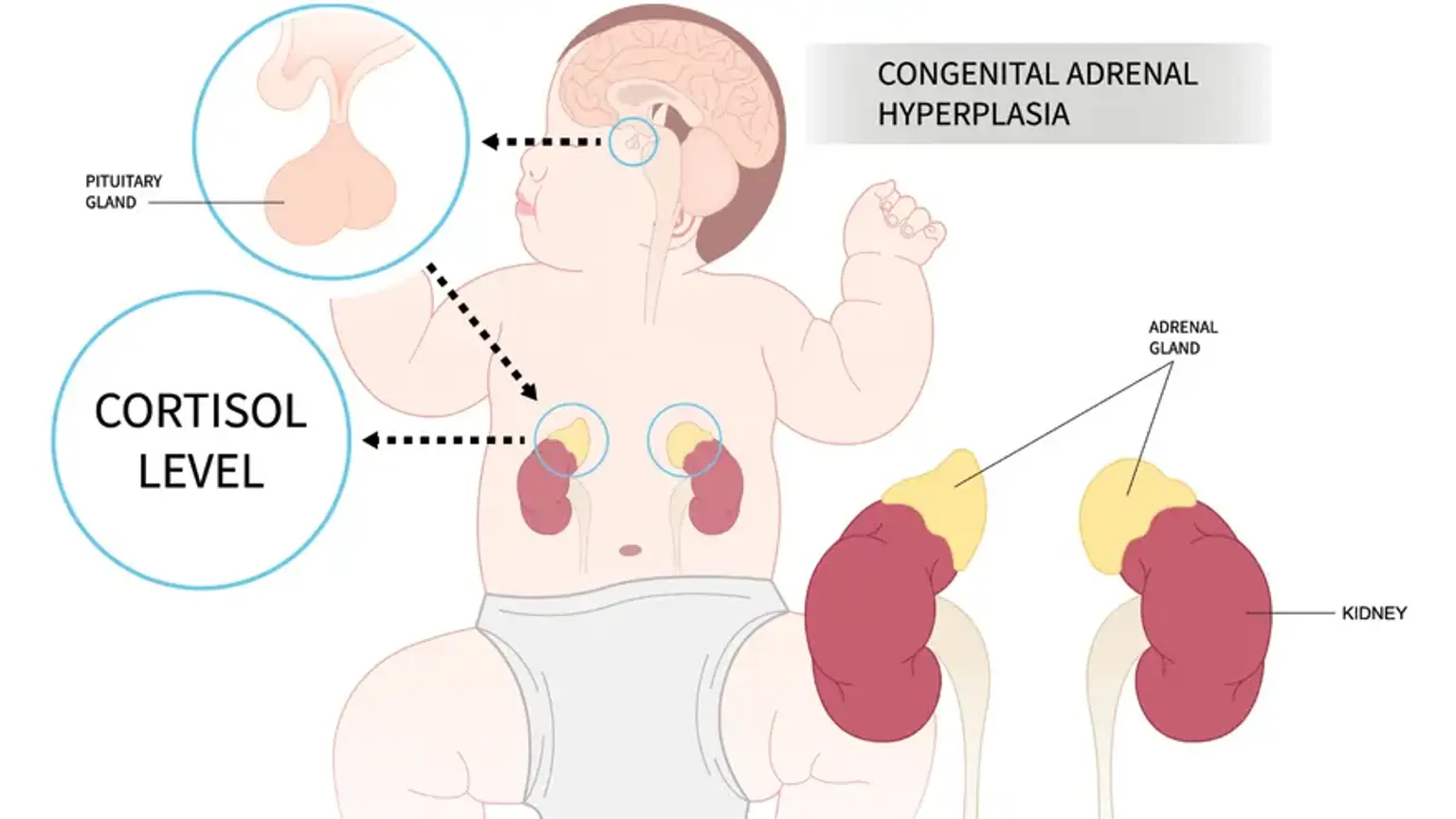
Congenital Adrenal Hyperplasia (CAH) is a group of inherited genetic disorders that affect the adrenal glands. These two small glands, located on top of the kidneys, are responsible for producing essential hormones like cortisol, aldosterone, and androgens. In individuals with CAH, a specific enzyme deficiency disrupts this hormone production. This condition affects approximately 1 in 15,000 to 1 in 18,000 births worldwide.This guide offers a comprehensive overview for patients, parents, and caregivers seeking to understand and manage this complex condition.
What is Congenital Adrenal Hyperplasia?
what-is-congenital-adrenal-hyperplasiaCongenital Adrenal Hyperplasia refers to a family of autosomal recessive genetic disorders. The core issue is a deficiency in one of the enzymes required to synthesize critical hormones in the adrenal cortex. The most common cause, accounting for over 95% of cases, is a deficiency of the enzyme 21-hydroxylase. When this enzyme is missing or deficient, the body cannot produce adequate amounts of cortisol, a hormone vital for regulating metabolism, blood sugar, and the body's response to stress and illness. In many cases, production of aldosterone, which regulates salt and water balance, is also impaired. The biochemical pathway is blocked, causing precursor molecules to be shunted towards the production of excess androgens male sex hormones, such as testosterone. This imbalance too little cortisol and aldosterone, and too much androgen is responsible for the diverse symptoms of CAH.
What are the different types of Congenital Adrenal Hyperplasia?
what-are-the-different-types-of-congenital-adrenal-hyperplasiaCAH is primarily classified into two major categories based on the severity of the enzyme deficiency.
Classic CAH: This is the more severe form and is usually detected during infancy or via newborn screening programs. It is further divided into two subtypes:
Salt-Wasting CAH: This is the most severe form. The enzyme deficiency is profound, leading to a critical lack of both cortisol and aldosterone. Without aldosterone, the body cannot retain sodium, leading to a life threatening salt wasting crisis.
Simple Virilizing CAH: In this form, enough aldosterone is produced to avoid a salt wasting crisis, but cortisol production is still deficient and androgen production is excessive. The primary characteristic is virilization development of masculine features.
Non-Classic CAH (NCAH): This is a milder, more common form. Individuals have a partial enzyme deficiency, allowing for some cortisol and aldosterone production. Symptoms are less severe and may not appear until late childhood, adolescence, or adulthood. NCAH often goes undiagnosed or is mistaken for other conditions like Polycystic Ovary Syndrome (PCOS).
What are the primary symptoms of CAH in infants and adults?
what-are-the-primary-symptoms-of-cah-in-infants-and-adultsThe signs and symptoms of CAH vary significantly depending on the type and the individual's age and sex.
In Infants with Classic CAH:
Ambiguous genitalia: Female infants often present with this at birth due to high androgen exposure in the womb. The clitoris may be enlarged, and the labia may be fused. The internal reproductive organs uterus, ovaries are normal.
Salt-wasting crisis: Occurs within the first few weeks of life in infants with the salt wasting form. Symptoms include poor feeding, vomiting, dehydration, low blood pressure, and lethargy. This is a medical emergency.
Normal-appearing genitalia in males: Male infants with classic CAH typically do not have ambiguous genitalia at birth, which can delay diagnosis if newborn screening is not performed.
In Children and Adolescents:
Early signs of puberty: Pubic hair, underarm hair, and acne can appear much earlier than normal.
Rapid growth: Children may be tall for their age initially, but their final adult height is often shorter because their bones mature too early.
In females: Irregular menstrual cycles, deepening voice, and development of facial hair hirsutism.
In Adults with Non-Classic CAH (NCAH):
Females: Often experience symptoms similar to PCOS, including hirsutism, severe acne, irregular or absent periods, and fertility problems.
Males: May experience early baldness, acne, or fertility issues, but many are asymptomatic.
What is a salt-wasting crisis in CAH?
what-is-a-salt-wasting-crisis-in-cahA salt-wasting crisis is the most dangerous complication of Classic CAH and is considered a medical emergency. It stems from a severe deficiency of the hormone aldosterone, which is crucial for instructing the kidneys to retain sodium salt.
Without sufficient aldosterone, the body rapidly loses sodium and water through urine, leading to:
Severe dehydration
Low blood sodium hyponatremia
High blood potassium hyperkalemia
Low blood pressure hypotension
Vomiting and poor feeding
Lethargy and, if untreated, shock and death.
This crisis typically occurs between one and four weeks of age. Immediate hospitalization is required for intravenous fluids containing salt and sugar, along with urgent administration of hormone medications.
How is Congenital Adrenal Hyperplasia diagnosed and confirmed?
how-is-congenital-adrenal-hyperplasia-diagnosed-and-confirmedThe diagnostic process for CAH involves several steps, often beginning before symptoms are even apparent.
Newborn Screening: Most developed countries screen for classic CAH using a blood spot test taken from the baby's heel. This test measures the level of 17-hydroxyprogesterone (17-OHP), a precursor that builds up when the 21-hydroxylase enzyme is deficient.
Blood Tests: If screening is positive or symptoms are present, further blood tests are ordered to measure levels of 17-OHP, cortisol, aldosterone, and androgens.
Genetic Testing: This is the definitive test to confirm the diagnosis. It identifies the specific gene mutations in the CYP21A2 gene, which is responsible for 21-hydroxylase deficiency.
ACTH Stimulation Test: This test is often used to diagnose the milder non-classic form (NCAH). A synthetic hormone (ACTH) is given to stimulate the adrenal glands, and blood levels of 17-OHP are measured before and after. An exaggerated response confirms the diagnosis.
Physical Examination: Evaluation of growth, development, and signs of excess androgen is a key part of the diagnostic process at any age.
What are the main treatments for managing CAH?
what-are-the-main-treatments-for-managing-cahWhile there is no cure for CAH, it is a manageable lifelong condition. The goal of treatment is to replace the deficient hormones and reduce excess androgen production.
Hormone Replacement Therapy: This is the foundation of CAH management.
Glucocorticoids: Medications like hydrocortisone for children or prednisone dexamethasone for adults are taken daily to replace cortisol. This replacement signals the pituitary gland to stop overstimulating the adrenals, which in turn reduces androgen production.
Mineralocorticoids: Patients with the salt wasting form must take fludrocortisone to replace aldosterone and normalize salt levels. They often require salt supplements as well, especially during infancy.
Stress Dosing: During times of significant physical stress such as fever, surgery, or major injury the body needs more cortisol. Patients must be taught to increase their glucocorticoid dose a stress dose to prevent an adrenal crisis, which is a life threatening condition caused by acute cortisol deficiency.
Surgical Interventions: For female infants born with significant virilization of the genitalia, feminizing genitoplasty may be considered. This is a complex and sensitive decision made in consultation with a multidisciplinary team of specialists, including pediatric endocrinologists and surgeons, and involves extensive counseling with the parents.
Regular Monitoring: Lifelong management requires regular follow up with an endocrinologist to monitor hormone levels, growth, and overall health, adjusting medication doses as needed.
"When our daughter was born, the doctors were confused. The diagnosis of classic CAH was terrifying at first, a storm of medical terms we didn't understand. But with the right team of endocrinologists, we learned how to manage her medication and what to do when she was sick. Seeing her thrive today is a testament to the power of a clear diagnosis and a consistent treatment plan." – An anonymous patient's family, South Korea.
When Should I See a Doctor for CAH?
when-should-i-see-a-doctor-for-cahPrompt medical evaluation is crucial. You should see a doctor if you observe:
In an infant: Ambiguous genitalia at birth, or signs of a salt wasting crisis vomiting, lethargy, poor feeding.
In a child: Early signs of puberty before age 8 in girls, age 9 in boys, such as pubic hair, rapid growth, or severe acne.
In an adolescent or adult female: Irregular or absent periods, excess facial or body hair hirsutism, severe acne, or difficulty conceiving.
In anyone diagnosed with CAH: Symptoms of an adrenal crisis, such as severe vomiting/diarrhea, high fever, or confusion. This requires emergency medical attention.
Recommended Clinics with Relevant Expertise in South Korea
recommended-clinics-with-relevant-expertise-in-south-koreaSouth Korea is home to world-class medical centers with highly specialized endocrinology and metabolism departments equipped to diagnose and manage complex conditions like Congenital Adrenal Hyperplasia.
Website | Clinic Name | Best Known For | Address | Contact |
|---|---|---|---|---|
Asan Medical Center | Endocrinology & Metabolism | Songpa-gu, Seoul, South Korea | ||
Seoul National University Hospital- ganganm district | Comprehensive Healthcare & Research | Gangnam-gu, Seoul, South Korea | ||
Severance Hospital | Endocrinology & Metabolism | Seodaemun-gu, Seoul, South Korea | ||
Seoul St. Mary's Hospital | Endocrinology & Metabolism | Seocho-gu, Seoul, South Korea | ||
Soon Chun Hyang University Bucheon Hospital | Endocrinology & Metabolism | Bucheon-si, Gyeonggi-do, South Korea | ||
Ewha Womans University Medical Center | Endocrinology & Metabolism | Gangseo-gu, Seoul, South Korea | ||
Cha University Bundang Medical Center | Endocrinology & Metabolism | Seongnam-si, Gyeonggi-do, South Korea | ||
Ulsan University Hospital | Endocrinology & Metabolism | Dong-gu, Ulsan, South Korea |
Recommended Treatment/Procedure Names with Average Costs in South Korea
recommended-treatmentprocedure-names-with-average-costs-in-south-koreaManagement of CAH is primarily medical. However, patients may require services from various endocrinology-related specialties. The costs below are estimates and vary based on the specific condition and treatment plan.
Treatment/Procedure Name | Duration | Hospitalization? | Avg. Cost (USD) in S.Korea? | Contact |
|---|---|---|---|---|
Adrenal Disorders Management | 1-2 visits | Not Needed | $100 - $400 | |
Reproductive Endocrinology (PCOS/Infertility) | 2 to 4 hours | Not Needed | $500 - $15,000 | |
Endocrine Hypertension Workup | 1-3 visits | Not Needed | $300 - $1,500 | |
Metabolic Bone Diseases (Osteoporosis) | 2 to 4 hours | Not Needed | $50 - $300 | |
Thyroidectomy for Thyroid Disorders | 1 to 2 hours | Needed (1 to 2 days) | $4,500 to $7,000 | |
Osteoporosis Infusion Therapy | 1 hour | Not Needed | $300 to $800 | |
Adrenalectomy for Adrenal Disorders | 2 to 4 hours | Needed (2 to 4 days) | $8,000 to $14,000 | |
Surgery for Pituitary Tumors | 3 to 4 hours | Needed (3 to 5 days) | $15,000 to $25,000 | |
IVF Cycle for PCOS or Infertility | 4 to 6 weeks | Not Needed | $4,000 to $7,000 | |
Endocrine Hypertension Diagnosis | 1 hour | Not Needed | $500 to $1,500 | |
Advanced Lipid Disorder Management | 30 min | Not Needed | $200 to $500 | |
Parathyroidectomy | 1 to 2 hours | Needed (1 day) | $6,000 to $10,000 | |
Pancreas Transplant | 4 to 6 hours | Needed (2 to 3 weeks) | $60,000 to $90,000 |
What Are Common Questions About Congenital Adrenal Hyperplasia?
what-are-common-questions-about-congenital-adrenal-hyperplasiaThis section addresses practical questions that patients and families often have.
1. Is Congenital Adrenal Hyperplasia hereditary?
1.-is-congenital-adrenal-hyperplasia-hereditaryYes. CAH is an autosomal recessive genetic disorder. This means that for a child to have CAH, they must inherit one copy of the mutated gene from each parent. The parents are typically carriers and do not have the condition themselves.
2. Can diet affect my condition?
2.-can-diet-affect-my-conditionThere is no special diet that can cure or treat CAH. However, a balanced, healthy diet is important for overall well-being. For individuals with the salt-wasting form, ensuring adequate salt intake is a critical part of management, especially during hot weather or illness.
3. Can CAH be cured permanently?
3.-can-cah-be-cured-permanentlyNo, CAH is a lifelong condition that cannot be cured. However, with consistent hormone replacement therapy and regular medical supervision, individuals with CAH can lead full, healthy, and productive lives.
4. Can adults be diagnosed with non-classic CAH?
4.-can-adults-be-diagnosed-with-non-classic-cahYes. It is common for non-classic CAH (NCAH) to be diagnosed in adolescence or adulthood. It is often discovered during an evaluation for symptoms like irregular periods, infertility, or severe acne that mimics PCOS.
5. How does CAH affect fertility and pregnancy?
5.-how-does-cah-affect-fertility-and-pregnancyExcess androgens can interfere with ovulation in women and sperm production in men, potentially causing infertility. With proper glucocorticoid treatment to control androgen levels, fertility can often be restored. Women with CAH require specialized care from an endocrinologist and obstetrician throughout pregnancy.
6. Are there new treatments being developed for CAH?
6.-are-there-new-treatments-being-developed-for-cahYes, research is ongoing. Scientists are developing modified release glucocorticoid preparations to better mimic the body's natural cortisol rhythm. Other potential therapies aiming to reduce androgen production without requiring high doses of steroids are also under investigation.
Take Control of Your Health: Get Expert Guidance for CAH Now!
take-control-of-your-health:-get-expert-guidance-for-cahManaging a complex condition like Congenital Adrenal Hyperplasia requires specialized, expert care. Whether you are seeking a diagnosis, a second opinion, or a long-term management plan, connecting with leading endocrinologists is the most important step. We provide a seamless, transparent process to access world-class care at South Korea's top medical centers. Your dedicated Care Manager will support you through every stage, from initial inquiry to post-treatment follow-up. Take the first step toward clarity and confidence in your health journey. Start Your Confidential Inquiry with CloudHospital and receive a personalized treatment plan from a leading specialist.