
The clinical information regarding Hiatal Hernia in this article has been rigorously verified against the latest guidance from authoritative bodies like the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and primary research from databases like PubMed. This piece was reviewed for accuracy and patient-centric clarity and was last updated in October 2023.
Introduction
introductionA hiatal hernia is a common anatomical condition, particularly in individuals over 50, yet it often goes undiagnosed. While many people live with a small hiatal hernia without any issues, for others it can cause significant discomfort and lead to chronic conditions like gastroesophageal reflux disease (GERD). This guide provides a comprehensive overview of what a hiatal hernia is, its causes, symptoms, and the full spectrum of modern treatment options, from lifestyle changes to advanced surgical procedures.
What is a Hiatal Hernia?
what-is-a-hiatal-hernia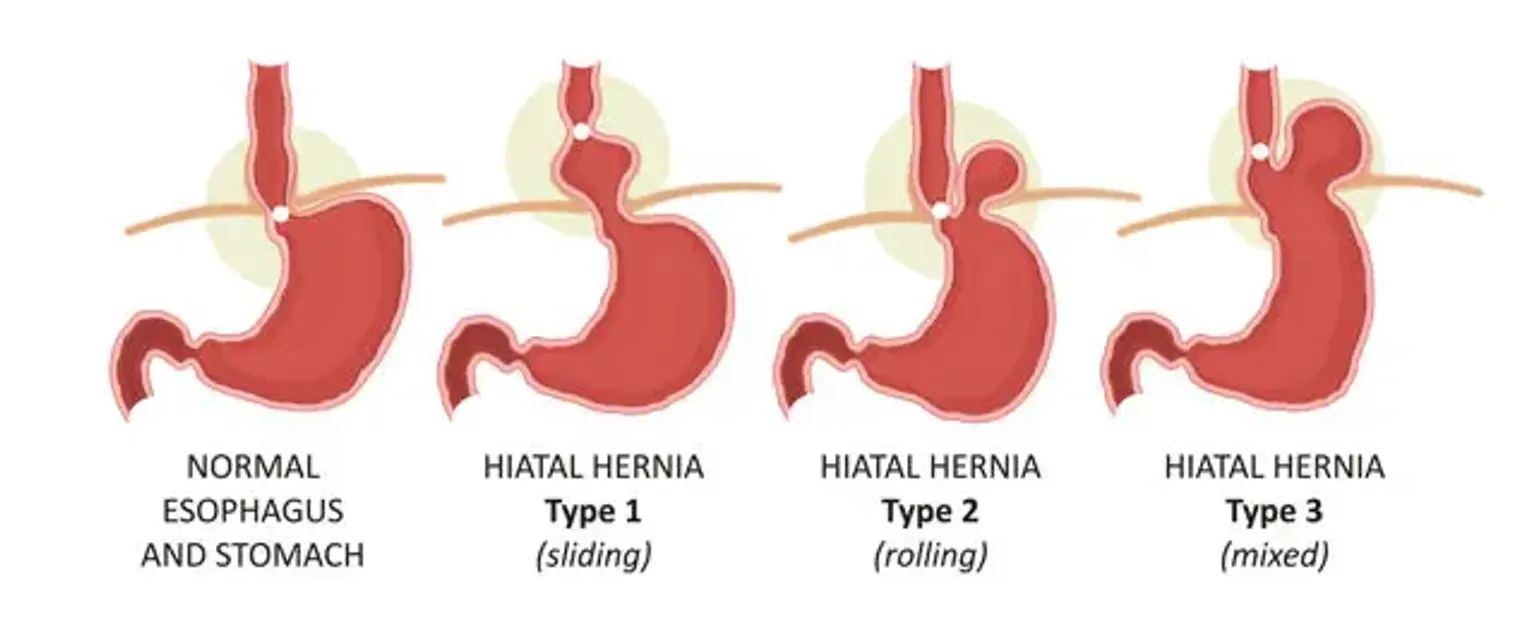
A hiatal hernia occurs when the upper part of your stomach bulges up through the large muscle separating your abdomen and chest the diaphragm. Your diaphragm has a small opening called the hiatus, through which your food tube the esophagus passes before connecting to your stomach. In a hiatal hernia, the stomach pushes up through this opening and into your chest.
There are two main types of hiatal hernias:
Sliding Hiatal Hernia (Type I): This is the most common type, accounting for over 95% of cases. The stomach and the section of the esophagus that joins the stomach slide up into the chest through the hiatus.
Paraesophageal Hiatal Hernia (Types II, III, IV): This type is less common but more concerning. The esophagus and stomach stay in their normal locations, but part of the stomach squeezes through the hiatus, landing it next to the esophagus. This type carries a risk of the stomach becoming strangulated, meaning the blood supply is cut off.
What are the Common Causes and Risk Factors for a Hiatal Hernia?
what-are-the-common-causes-and-risk-factors-for-a-hiatal-herniaA hiatal hernia is caused by weakened muscle tissue that allows your stomach to bulge up through your diaphragm. The exact reason for this weakening is not always known, but several factors can increase your risk:
Age-related changes: The diaphragm can weaken with age, making older adults more susceptible.
Increased pressure: Intense and persistent pressure on the muscles around the stomach can contribute. This pressure can come from:
Chronic coughing or vomiting
Straining during bowel movements
Heavy lifting or strenuous physical activity
Pregnancy
Obesity
Injury or Surgery: Previous injury to the area or certain types of surgery can increase the risk.
Genetics: Some individuals may be born with an unusually large hiatus.
What are the First Signs and Symptoms of a Hiatal Hernia?
what-are-the-first-signs-and-symptoms-of-a-hiatal-herniaMany small hiatal hernias cause no signs or symptoms. However, larger hernias can allow food and stomach acid to back up into your esophagus, leading to a range of symptoms, including:
Heartburn: A burning sensation in your chest that can worsen after eating or when lying down.
Regurgitation: The backflow of food or liquid into your mouth.
Acid Reflux: A sour or bitter taste at the back of your throat.
Difficulty Swallowing Dysphagia: A feeling that food is stuck in your chest.
Chest or Abdominal Pain: Pain that can be mistaken for a heart attack.
Shortness of Breath: A large hernia can press on the lungs.
Belching or Bloating: Feeling full soon after you start eating.
How is a Hiatal Hernia Diagnosed?
how-is-a-hiatal-hernia-diagnosedIf you experience persistent symptoms, a gastroenterologist will perform a thorough evaluation. The diagnostic process typically involves several steps to confirm the presence and type of hernia.
Medical History and Physical Exam: Your doctor will first discuss your symptoms, diet, and lifestyle.
Upper GI Endoscopy (EGD): This is a primary diagnostic tool. A thin, flexible tube with a camera endoscope is passed down your throat to view your esophagus and stomach. This allows the doctor to see the hernia directly.
Barium Swallow (Esophagram): For this test, you drink a chalky liquid containing barium that coats your upper digestive tract. X-rays are then taken, which provides a clear silhouette of your esophagus, stomach, and the location of the hernia.
Esophageal Manometry: This test measures the rhythmic muscle contractions in your esophagus when you swallow. It assesses the function and coordination of the esophageal muscles and the lower esophageal sphincter.
pH Monitoring: This test can measure the amount of acid in your esophagus over a 24-48 hour period to confirm if symptoms are related to GERD.
What are the Treatment Options for a Hiatal Hernia?
what-are-the-treatment-options-for-a-hiatal-herniaTreatment depends on the severity of your symptoms and the type of hernia. Many people find relief with conservative management, while others may require surgery.
Lifestyle Modifications and Medications
lifestyle-modifications-and-medicationsFor sliding hernias with mild symptoms, the first line of treatment focuses on managing acid reflux.
Dietary Changes: Avoiding trigger foods like citrus, tomatoes, fatty foods, chocolate, mint, alcohol, and caffeine.
Lifestyle Adjustments: Eating smaller, more frequent meals; not lying down for at least three hours after eating; elevating the head of your bed; and losing weight if overweight.
Medications:
Antacids: Over the counter options to neutralize stomach acid.
H2-receptor blockers: Reduce acid production.
Proton pump inhibitors (PPIs): Stronger acid blockers that also allow esophageal tissue time to heal.
Surgical Interventions
surgical-interventionsSurgery is typically recommended when medications and lifestyle changes are not effective, or for paraesophageal hernias that pose a risk of complications. The primary goal of surgery is to pull the stomach back into the abdomen and make the opening in the diaphragm smaller.
Laparoscopic Nissen Fundoplication: This is the most common surgical procedure. The surgeon makes several small incisions in the abdomen and uses specialized instruments to wrap the top of the stomach the fundus around the lower esophagus. This tightens the lower esophageal sphincter to prevent reflux. Most of these are performed laparoscopically, which ensures a faster recovery.
Hernia Repair: In all surgical cases, the surgeon will repair the hiatal hernia by repositioning the stomach into the abdominal cavity and reinforcing the hiatal opening with stitches or a synthetic mesh.
Can a Hiatal Hernia Be Cured Without Surgery?
can-a-hiatal-hernia-be-cured-without-surgery"For years, I thought the constant, gnawing heartburn and the scary feeling of food getting stuck in my chest was just something I had to live with. Getting a clear diagnosis of a hiatal hernia and starting a targeted treatment plan gave me my life back." – an anonymous patient, South Korea.
While lifestyle changes and medications can effectively manage the symptoms of a sliding hiatal hernia, they do not cure the physical hernia itself. The anatomical defect the stomach pushing through the diaphragm remains. For many, symptom management is sufficient for a high quality of life. However, surgery is the only method to physically correct the hernia and provide a potential permanent cure, especially for those with severe, debilitating symptoms or a paraesophageal hernia.
When Should I See a Doctor for Hiatal Hernia Symptoms?
when-should-i-see-a-doctor-for-hiatal-hernia-symptomsYou should schedule an appointment with a healthcare professional if you experience persistent or severe symptoms like heartburn, regurgitation, or difficulty swallowing.
Seek immediate medical attention if you experience:
Severe chest or abdominal pain
Inability to have a bowel movement or pass gas
Nausea and vomiting
These could be signs of hernia obstruction or strangulation, which are medical emergencies.
Recommended Clinics with Relevant Expertise in South Korea
recommended-clinics-with-relevant-expertise-in-south-koreaSouth Korea is home to world-class medical centers with advanced gastroenterology departments skilled in diagnosing and treating complex digestive conditions like hiatal hernias.
Website | Clinic Name | Best Known For | Address | Contact |
|---|---|---|---|---|
Asan Medical Center | Comprehensive care in Endocrinology & Metabolism, advanced diabetes management | Songpa-gu, Seoul, South Korea | ||
Seoul National University Hospital- Gangnam district | Executive health screenings, specialized endocrine disorder management | Gangnam-gu, Seoul, South Korea | ||
Severance Hospital | Leading research in diabetes, pituitary and thyroid disorders | Seodaemun-gu, Seoul, South Korea | ||
Seoul St. Mary's Hospital-Seocho | Islet cell and pancreas transplantation, metabolic diseases | Seocho-gu, Seoul, South Korea | ||
Soon Chun Hyang University Bucheon Hospital | Specialized care in Endocrinology & Metabolism for Gyeonggi province | Bucheon-si, Gyeonggi-do, South Korea | ||
Ewha Womans University Medical Center | Expertise in female-specific endocrine disorders like PCOS and thyroid issues | Seodaemun-gu, Seoul, South Korea | ||
Cha University Bundang Medical Center | Strong focus on reproductive endocrinology and metabolic syndromes | Gyeonggi-do, Bundang-gu, Seongnam-si, South Korea | ||
Ulsan University Hospital | Regional center for endocrine disorders, including diabetes and thyroid cancer | Dong-gu, Ulsan, South Korea |
Recommended Treatment/Procedure Names with Average Costs in South Korea
recommended-treatmentprocedure-names-with-average-costs-in-south-koreaThe following are common gastroenterological procedures, some of which are used in the diagnosis or treatment of hiatal hernias and related conditions. Costs are estimates and can vary based on the specifics of the case and hospital.
Treatment/Procedure Name | Duration | Hospitalization? | Avg. Cost(USD) in S. Korea? | Contact |
|---|---|---|---|---|
Endoscopic Ultrasound (EUS) with Fine Needle Aspiration | 30-60 minutes | Not Needed | $2,500 - $5,000 | |
Bariatric Surgery (Gastric Bypass, Sleeve Gastrectomy) | 1-3 hours | Needed (2-4 days) | $9,000 - $16,000 | |
Colon Cancer Surgery (Colectomy) | 2-4 hours | Needed (3-7 days) | $15,000 - $25,000 | |
Inflammatory Bowel Disease (IBD) Biologic Therapy | 30 mins - 2 hours | Not Needed | $1,000 - $5,000 | |
Upper GI Endoscopy with Biopsy (EGD) | 15-30 minutes | Not Needed | $800 - $1,500 | |
Colonoscopy with Polypectomy | 30-60 minutes | Not Needed | $1,000 - $2,000 | |
Pancreatic Surgery (Whipple Procedure) | 4-8 hours | Needed (1-2 weeks) | $40,000 - $70,000 | |
Hepatitis C Antiviral Therapy | 8-12 week | Not Needed | $20,000 - $40,000 |
What Are Common Questions About a Hiatal Hernia?
what-are-common-questions-about-a-hiatal-herniaThis section addresses practical questions patients often have about living with this condition.
1. What is the recovery time for hiatal hernia surgery?
1.-what-is-the-recovery-time-for-hiatal-hernia-surgeryFor a laparoscopic procedure, most patients can return to office work and light activities within 1 to 2 weeks. Full recovery and a return to strenuous activities may take 4 to 6 weeks. You will be on a modified diet, starting with liquids and gradually progressing to soft foods, for several weeks post-surgery.
2. What foods should be avoided with a hiatal hernia?
2.-what-foods-should-be-avoided-with-a-hiatal-herniaTo manage symptoms, it is best to avoid foods that trigger acid reflux. These commonly include:
Fried, greasy, or high-fat foods
Spicy foods
Acidic fruits and vegetables like oranges, lemons, and tomatoes
Onions and garlic
Chocolate and peppermint
Carbonated beverages, coffee, and alcohol
3. Is a sliding hiatal hernia dangerous?
3.-is-a-sliding-hiatal-hernia-dangerousA sliding hiatal hernia is generally not considered dangerous on its own. The primary concern is the chronic GERD it can cause, which, if left untreated over many years, can lead to complications like inflammation of the esophagus esophagitis, narrowing of the esophagus strictures, and a precancerous condition known as Barrett's esophagus.
4. How do you fix a hiatal hernia?
4.-how-do-you-fix-a-hiatal-herniaA hiatal hernia can only be physically fixed with surgery. The procedure involves moving the stomach back into the abdominal cavity and tightening the hiatal opening in the diaphragm. For many, however, the symptoms can be effectively fixed or managed long-term with medication and lifestyle adjustments.
5. Can a hiatal hernia cause heart palpitations?
5.-can-a-hiatal-hernia-cause-heart-palpitationsYes, in some cases, a large hiatal hernia can irritate the vagus nerve, which runs through the chest and plays a role in regulating heart rate. This irritation can sometimes lead to heart palpitations or a feeling of a racing or irregular heartbeat, especially after a large meal. It is crucial to have any chest-related symptoms evaluated by a doctor to rule out a cardiac cause.
6. Can exercise make a hiatal hernia worse?
6.-can-exercise-make-a-hiatal-hernia-worseCertain types of exercise, particularly those that increase intra abdominal pressure like heavy weightlifting, crunches, or abdominal presses, can potentially worsen symptoms. However, moderate, low-impact exercise like walking, swimming, and cycling is generally safe and encouraged, especially for weight management.
7. Does stress affect a hiatal hernia?
7.-does-stress-affect-a-hiatal-herniaStress doesn't cause a hiatal hernia, but it can worsen the symptoms. High stress levels can increase stomach acid production and heighten your perception of pain, making heartburn and reflux feel more severe.
Find Lasting Relief from Hiatal Hernia: Begin Your Treatment Journey Now!
find-lasting-relief-from-hiatal-hernia:-begin-your-treatment-journeyYou don’t have to live with the discomfort of a hiatal hernia or GERD. South Korea’s top medical centers offer advanced diagnosis and treatment options. With CloudHospital, you’ll receive expert support and a dedicated Care Manager to guide you through every step from consultation to recovery. Start Your Confidential Inquiry and receive a free, personalized treatment plan from leading specialists.