
The clinical information regarding Chlamydia in this article has been rigorously verified against the latest 2021 STI Treatment Guidelines from the Centers for Disease Control and Prevention CDC and primary research from databases like PubMed. This piece was reviewed for accuracy and patient-centric clarity and was last updated in September 2023.
Introduction
introductionChlamydia is one of the most common sexually transmitted infections STIs globally, with an estimated 129 million new cases among adults each year. Because it often presents with no symptoms, many individuals are unaware they have it, increasing the risk of transmission and long term health complications. This guide offers a comprehensive, medically grounded overview for those seeking to understand, diagnose, and treat Chlamydia effectively.
What is Chlamydia?
what-is-chlamydia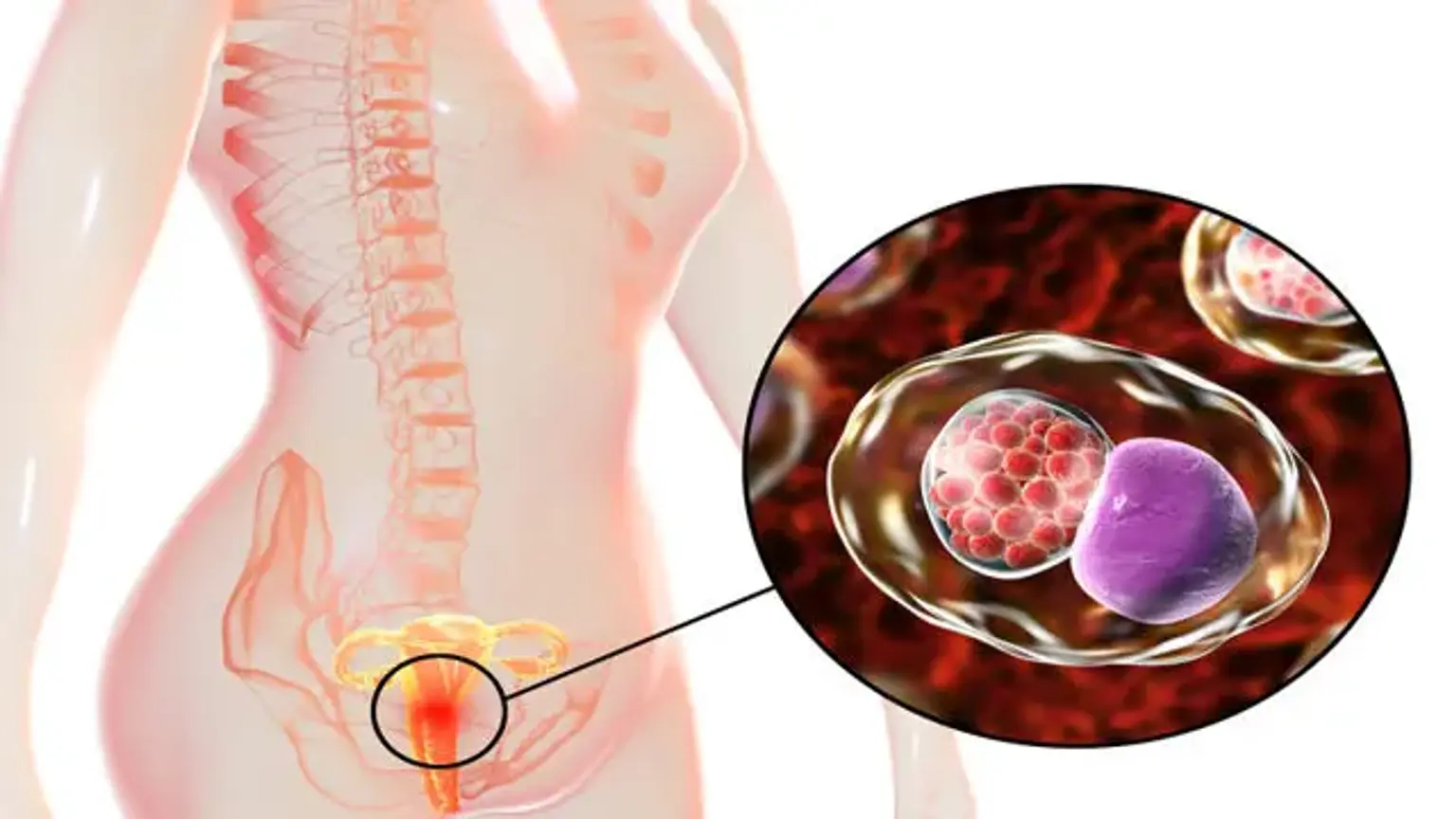
Chlamydia is a bacterial infection caused by Chlamydia trachomatis. This bacterium primarily infects the cells of the cervix, urethra, and rectum. It can also infect the throat and the eyes. The infection is highly transmissible through sexual contact. If untreated, it can lead to serious and permanent damage to a woman's reproductive system, making it a significant public health concern.
What are the early signs of Chlamydia in women?
what-are-the-early-signs-of-chlamydia-in-womenThe majority of Chlamydia infections are asymptomatic, meaning they produce no noticeable signs, which is why it is often called a silent infection. When symptoms do appear, they typically start one to three weeks after exposure and can be mild.
Key potential symptoms include:
An abnormal vaginal discharge that may be yellow and have a strong odor
A burning sensation during urination
Pain during sexual intercourse
Bleeding between menstrual periods or after sex
Lower abdominal pain or pelvic pain
Rectal pain, discharge, or bleeding
How is Chlamydia transmitted between partners?
how-is-chlamydia-transmitted-between-partnersChlamydia is primarily transmitted through sexual contact with an infected partner. This includes vaginal, anal, and oral sex. The bacteria can be passed even if a male partner does not ejaculate. It can also be spread from an infected mother to her baby during childbirth, potentially causing eye infections or pneumonia in the newborn. It is not spread through casual contact such as kissing, hugging, or sharing toilets.
How is Chlamydia Diagnosed?
how-is-chlamydia-diagnosedDiagnosing Chlamydia is a straightforward process conducted by a healthcare professional, usually a gynaecologist. Early and accurate diagnosis is critical to prevent complications.
The primary diagnostic methods include:
Nucleic Acid Amplification Tests NAAT: These are the most sensitive tests for Chlamydia. A healthcare provider will take a urine sample or a swab from the cervix in women or the urethra in men. These samples are then analyzed in a lab to detect the genetic material of the Chlamydia bacteria.
Pelvic Exam: A doctor may perform a pelvic exam to check for signs of infection such as inflammation or abnormal discharge. During this exam, a swab sample is often collected for testing.
Regular screening is recommended for sexually active women under 25 and for older women with new or multiple sexual partners, as early detection in asymptomatic cases is vital.
What is the most effective treatment for Chlamydia?
what-is-the-most-effective-treatment-for-chlamydiaThe most effective treatment for Chlamydia is a course of antibiotics prescribed by a doctor. Chlamydia is highly curable with the correct medication. It is crucial to take the full course of antibiotics as prescribed, even if symptoms improve or disappear before the medication is finished.
The two most commonly prescribed antibiotic regimens are:
Azithromycin: Typically given as a single, one gram oral dose.
Doxycycline: Usually prescribed as a 100 milligram pill taken twice a day for seven days. This regimen has a slightly higher cure rate.
Patients should abstain from sexual contact for seven days after completing a single dose of azithromycin or until they have finished the full seven day course of doxycycline to prevent spreading the infection.
What happens if Chlamydia is left untreated?
what-happens-if-chlamydia-is-left-untreatedIf Chlamydia is not treated, it can cause severe and irreversible health problems, particularly for women. The infection can spread from the cervix to the upper reproductive tract, including the uterus and fallopian tubes.
Major complications include:
Pelvic Inflammatory Disease PID: This is a serious infection of the female reproductive organs. PID can cause chronic pelvic pain, scar tissue formation, and damage to the fallopian tubes.
Infertility: Scarring from PID can block the fallopian tubes, preventing eggs from traveling to the uterus and thus causing infertility.
Ectopic Pregnancy: If a fallopian tube is partially blocked by scar tissue, a fertilized egg may implant outside the uterus, most often in the tube itself. This is a life threatening condition that requires immediate medical intervention.
Reactive Arthritis: A small percentage of people with Chlamydia may develop this condition, which causes joint pain, inflammation of the eyes, and inflammation of the urinary tract.
How can I manage my sexual health after a diagnosis?
how-can-i-manage-my-sexual-health-after-a-diagnosisReceiving a diagnosis can be concerning, but it is the first step toward protecting your long term health. It is essential to inform all sexual partners from the previous 60 days so they can be tested and treated. This action prevents reinfection and stops the spread of the infection to others. After treatment, a follow up test, known as a test of cure, is often recommended about three months later to ensure the infection is gone and you have not been reinfected.
"The worst part was not knowing. I had some mild discomfort but dismissed it. Getting the diagnosis was a shock, but the treatment was so simple. The peace of mind I felt after getting treated and knowing I was protecting my future health was immense." – an anonymous patient, South Korea.
When Should I See a Doctor for Chlamydia?
when-should-i-see-a-doctor-for-chlamydiaYou should see a doctor immediately if you experience any symptoms of Chlamydia, such as abnormal discharge, pain during urination, or pelvic pain. Furthermore, it is critical to get tested if a current or former sexual partner informs you they have tested positive for Chlamydia. Due to the high rate of asymptomatic infections, sexually active individuals, especially those under 25 or with new partners, should discuss regular STI screening with their gynaecologist as part of their routine healthcare.
Recommended Clinics with Relevant Expertise in South Korea
recommended-clinics-with-relevant-expertise-in-south-koreaWebsite | Clinic Name | Best Known For | Address | Contact |
|---|---|---|---|---|
Second Spring Women's Clinic | Comprehensive Women's Health and Maternity Care | Gangnam-gu, Seoul, South Korea | ||
Seoul Miz Hospital | Gynecological Surgery, Vaginal Aesthetic Treatments | Gangdong-gu, Seoul, South Korea | ||
MariaPlus Fertility Hospital | Advanced Fertility Treatments and Reproductive Medicine | Songpa-gu, Seoul, South Korea | ||
Asan Medical Center | World Class Multispecialty Hospital, including OBGYN | Songpa-gu, Seoul, South Korea | ||
Goeunbit Women’s Clinic | Women's Disease and Menopause Management | Songpa-gu, Seoul, South Korea | ||
MizMedi Hospital | Specialized in Women's and Children's Health | Gangseo-gu, Seoul, South Korea | ||
HI Fertility Clinic | High Success Rate Fertility and IVF Procedures | Gangseo-gu, Seoul, South Korea | ||
Helen Women’s Obstetrics & Gynecology Clinic | Contraception and Menstrual Disorder Treatments | Songpa-gu, Seoul, South Korea |
Recommended Treatment/Procedure Names with Average Costs in South Korea
recommended-treatmentprocedure-names-with-average-costs-in-south-koreaTreatment/Procedure Name | Duration | Hospitalization? | Avg. Cost (USD) in S. Korea | Contact |
|---|---|---|---|---|
Chlamydia NAAT Test Urine or Swab | 5 to 10 mins | Not Needed | $50 to $150 | |
Pelvic Exam | 10 to 15 mins | Not Needed | $100 to $250 | |
Transvaginal Ultrasound for PID | 15 to 30 mins | Not Needed | $200 to $400 | |
Diagnostic Laparoscopy for PID | 30 to 60 mins | Needed (1 day) | $2,500 to $5,000 | |
Hysterosalpingography HSG | 15 to 30 mins | Not Needed | $400 to $800 | |
Endometrial Biopsy | 10 to 15 mins | Not Needed | $300 to $600 | |
In Vitro Fertilization IVF | 4 to 6 weeks | Not Needed | $9,000 to $15,000 | |
Surgical Adhesiolysis | 1 to 2 hours | Needed (1 to 2 days) | $4,000 to $7,000 |
What Are Common Questions About Chlamydia?
what-are-common-questions-about-chlamydia1. Can Chlamydia cause permanent infertility?
1.-can-chlamydia-cause-permanent-infertilityYes, Chlamydia can cause permanent infertility in women if it is left untreated. The infection can lead to Pelvic Inflammatory Disease PID, which creates scar tissue that blocks the fallopian tubes, preventing conception. Early treatment is the best way to prevent this complication.
2. How long does it take to cure Chlamydia with antibiotics?
2.-how-long-does-it-take-to-cure-chlamydia-with-antibioticsChlamydia is cured after you complete the full course of prescribed antibiotics. For a single dose of azithromycin, the infection is typically cleared within seven days. For a seven day course of doxycycline, the infection is cleared once the full course is finished.
3. Is Chlamydia testing painful for women?
3.-is-chlamydia-testing-painful-for-womenNo, Chlamydia testing is generally not painful. The most common methods are a simple urine test or a gentle swab of the cervix, similar to a Pap test. While a cervical swab might cause momentary discomfort for some, it is not considered a painful procedure.
4. Can you get Chlamydia more than once?
4.-can-you-get-chlamydia-more-than-onceYes, you can be reinfected with Chlamydia. Having the infection once does not make you immune. This is why it is crucial for all sexual partners to be treated simultaneously and to practice safe sex to prevent reinfection.
5. Do I need to tell my past partners if I test positive?
5.-do-i-need-to-tell-my-past-partners-if-i-test-positiveYes, it is very important to notify any person you have had sex with in the 60 days prior to your diagnosis. This process, called partner notification, is essential for their health and helps to stop the ongoing spread of the infection in the community.
6. Is Chlamydia related to HPV or herpes?
6.-is-chlamydia-related-to-hpv-or-herpesNo, Chlamydia is a bacterial infection caused by Chlamydia trachomatis. HPV Human Papillomavirus and herpes are viral infections. While all are STIs, they are caused by different types of pathogens and require different methods of diagnosis, treatment, and management.
Take Control of Your Sexual Health: Get Confidential Answers Today!
take-control-of-your-sexual-health:-get-confidential-answers-todayNavigating a potential STI diagnosis can be stressful, but you do not have to do it alone. The first step towards peace of mind and long term health is getting clear, confidential, and expert medical advice. The clinics listed above, in partnership with CloudHospital, are leaders in women's health in South Korea, offering a safe and supportive environment for testing and treatment. We provide a seamless, transparent process with a dedicated Care Manager to support you from your initial inquiry to your post recovery care. And Start Your Confidential Inquiry today.