Introduction
ACL (anterior cruciate ligament) reconstruction surgery is a common procedure used to treat torn or damaged ACLs in the knee. The ACL plays a vital role in stabilizing the knee joint, especially during activities involving sudden stops, twists, or jumps—such as in soccer, basketball, and skiing. ACL injuries are prevalent, particularly among athletes, but can also result from general trauma or accidents.
When an ACL tear occurs, it often leads to knee instability, making it difficult to walk, run, or participate in sports. This is where ACL reconstruction comes in: a surgical approach aimed at restoring the ligament's function. The procedure typically involves replacing the torn ACL with a graft, which can be taken from the patient's own body or a donor. It is a minimally invasive surgery that allows most patients to return to normal activities after a period of rehabilitation.
What is ACL Reconstruction Surgery?
ACL reconstruction is a surgical procedure designed to repair or replace a torn ACL in the knee. The surgery involves removing the damaged ligament and replacing it with a graft, which helps restore the knee's stability and function. This procedure is essential when a torn ACL leads to knee instability that cannot be managed with non-surgical treatments like physical therapy or bracing.
During the procedure, the surgeon uses small incisions to insert an arthroscope—a small camera that allows them to view the knee joint and guide the surgery. The torn ACL is removed, and a graft is inserted to take its place. This can either be from the patient's own tissue (autograft) or from a donor (allograft). Once the graft is in place, the knee is secured and rehabilitation begins.
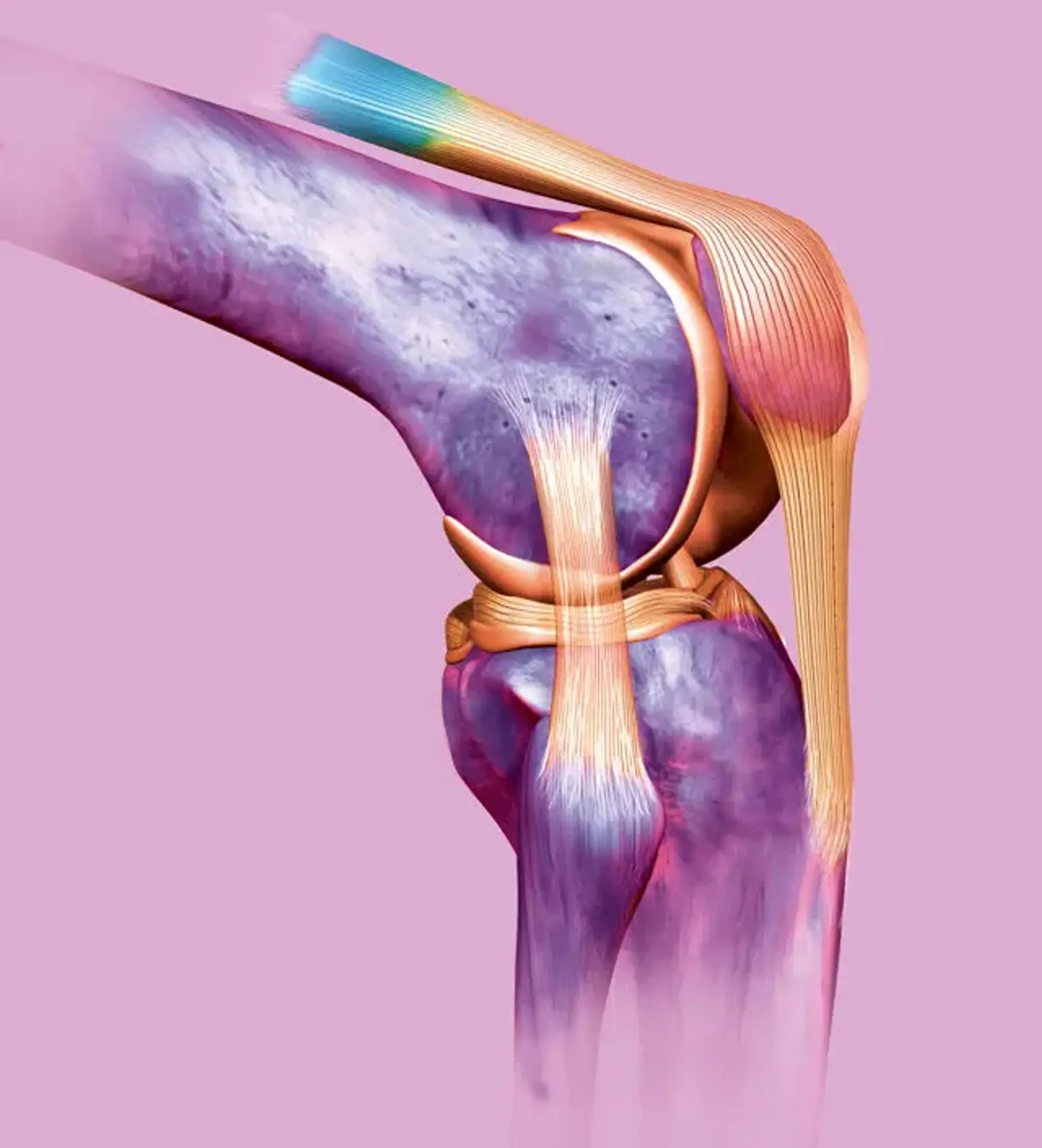
The Anatomy of the ACL
The ACL is a crucial ligament in the knee that connects the femur (thigh bone) to the tibia (shin bone). It controls the movement of the knee, particularly in preventing the tibia from sliding too far forward under the femur. It also provides rotational stability during activities like pivoting or cutting.
When the ACL is torn, the knee loses its ability to stabilize properly, especially during high-demand activities. This instability can lead to further damage to the knee joint, including damage to other structures like the meniscus (cartilage) and articular cartilage. ACL reconstruction surgery aims to restore this stability and prevent further joint damage.
When is ACL Reconstruction Surgery Necessary?
ACL reconstruction surgery becomes necessary when a torn ACL causes persistent knee instability, especially if conservative treatments (like physical therapy or bracing) fail to provide sufficient support. The decision to undergo surgery often depends on the severity of the injury, the patient's activity level, and their long-term goals.
For active individuals, especially athletes, ACL reconstruction is often the best option to return to sports safely. However, if the tear is minor and the knee remains stable, non-surgical approaches might be considered. ACL surgery is also recommended for patients who experience recurrent knee buckling or instability, which can interfere with daily activities and increase the risk of further injury.
Understanding the Surgical Procedure
ACL reconstruction surgery is typically performed using minimally invasive techniques, such as arthroscopy. The surgeon makes small incisions around the knee, through which a camera (arthroscope) and specialized surgical tools are inserted. This allows for a clearer view of the knee joint without the need for large, open incisions, promoting quicker recovery and less post-surgical discomfort.
The first step in the procedure is to remove the damaged ACL. The surgeon then prepares the site for the graft, which will replace the torn ligament. The graft can be taken from the patient’s own body (autograft) or a donor (allograft). After harvesting the graft, the surgeon secures it into the knee, typically using screws or other fixation devices. The new ligament restores knee stability, allowing for the return of normal function.
Types of Grafts Used in ACL Reconstruction
There are several options for grafts used in ACL reconstruction surgery. The most common types include:
Autograft: This graft is taken from the patient's own body, usually from the patellar tendon (located below the kneecap), hamstring tendon, or quadriceps tendon. Autografts are often preferred due to their lower risk of rejection and better integration with the knee.
Allograft: This graft is taken from a donor. Allografts are typically used when an autograft is not feasible or preferred. While they carry a slightly higher risk of infection or rejection, they can be a good option for older patients or those who require a quicker recovery.
Synthetic Grafts: These are man-made materials used as substitutes for biological grafts. Although still under investigation, synthetic grafts offer a promising alternative for ACL reconstruction, particularly in cases where biological grafts are not viable.
The choice of graft depends on factors such as the patient’s age, activity level, and the surgeon’s recommendation.
Risks and Complications of ACL Reconstruction
Like any surgery, ACL reconstruction carries certain risks. While the procedure is generally safe, complications can occur, including:
Infection: Though rare, an infection can occur at the incision sites or within the knee joint. This may require antibiotics or additional surgery.
Graft Failure: In some cases, the graft may not heal properly or could fail over time, especially if the patient returns to strenuous activities too soon.
Blood Clots: Post-surgery, blood clots can form in the legs or lungs, which is why early mobilization and blood thinners are often recommended.
Knee Stiffness or Instability: While ACL reconstruction aims to restore knee function, some patients may experience stiffness or feel that their knee is still unstable after surgery.
While these risks are present, the benefits of ACL reconstruction in restoring knee function and enabling a return to daily activities or sports often outweigh the potential complications. Proper rehabilitation and adherence to post-surgery guidelines can reduce these risks significantly.
How Long Does It Take to Recover from ACL Surgery?
Recovery from ACL surgery typically spans 6 to 12 months, with the exact timeline depending on factors such as the patient's age, graft type, and adherence to rehabilitation protocols. In the early stages, patients will focus on reducing swelling and restoring knee mobility.
By 6 weeks, most patients can resume light activities, but more intense physical activities, including sports, are usually not recommended until 6 to 12 months after surgery. Athletes often follow a structured return-to-play protocol to ensure they are fully healed and the knee is stable.
Patience is key, as pushing recovery too quickly can risk re-injury. A gradual, consistent approach to rehabilitation is essential for a successful outcome.
Recovery and Rehabilitation After ACL Surgery
The recovery process after ACL surgery can be lengthy but essential for achieving the best possible outcome. After surgery, the knee will be swollen, and some pain is expected. Most patients are able to walk with the help of crutches within a few days.
The rehabilitation process is crucial for regaining strength, mobility, and stability in the knee. Physical therapy typically begins shortly after surgery and progresses through three phases:
Phase 1 (0-2 weeks): The focus is on reducing swelling and pain, while starting gentle range-of-motion exercises.
Phase 2 (2-6 weeks): As the knee heals, strengthening exercises are introduced to help restore muscle function, particularly in the quadriceps and hamstrings.
Phase 3 (6-12 weeks): Increased intensity in rehabilitation exercises, including sport-specific drills if the patient is an athlete, to prepare for a return to activity.
Full recovery can take anywhere from 6 to 12 months, depending on the individual’s healing progress and adherence to rehabilitation. It’s essential to follow the physical therapist’s instructions carefully to ensure the graft heals properly and the knee becomes stable enough for regular activities.
Pediatric and Adolescent ACL Reconstruction
ACL injuries in children and adolescents present unique challenges due to the ongoing growth of their bones and the potential for growth plate damage. For younger patients, the surgery needs to be carefully planned to avoid harm to these growth plates.
ACL reconstruction in pediatric patients often involves techniques designed to protect the growth plates, such as the "All-Epiphyseal" method, which uses a graft without disturbing the growth areas. Recovery for younger patients can take longer, but the goal is to enable a return to sports with minimal risk of re-injury or growth disruption.
Athletic participation should be carefully monitored in these cases to ensure safe healing while preventing future injuries.
ACL Reconstruction in Athletes
For athletes, ACL reconstruction is often essential to return to high-performance sports. An ACL tear can drastically affect an athlete's ability to pivot, jump, or change direction, making the surgery crucial for restoring function.
Athletes typically undergo more intense rehabilitation to regain strength and mobility. The goal is not just to return to normal activity, but to return to competitive sports at the highest level. Studies show that with proper rehabilitation, athletes can return to their sport, often at the same level of performance.
The key to a successful return is ensuring that the knee is fully healed and stable, and that the athlete follows a structured rehabilitation program that mimics the demands of their sport.
Revision ACL Surgery
In some cases, a first-time ACL reconstruction may fail, requiring revision surgery. Revision ACL surgery is typically needed if the graft fails, the knee becomes unstable again, or if the patient sustains another tear. This surgery is more complex than the initial procedure due to scar tissue and the need to use different grafts or surgical techniques.
The success rates of revision ACL surgery depend on factors such as the surgeon's experience, the cause of the original failure, and the patient’s rehabilitation. The recovery process for revision surgery may take longer, and the risks are higher, but many patients still successfully return to their previous levels of activity.
Innovations and Advancements in ACL Surgery
ACL reconstruction has seen significant advancements in recent years. One of the major innovations is robot-assisted surgery, which enhances precision during the procedure, leading to more accurate graft placement and potentially faster recovery times.
Another key advancement is the development of enhanced grafts, including synthetic ligaments and biologic grafts, which promote faster healing and reduce the risk of rejection. These newer materials are being studied for their ability to mimic the natural ACL more closely.
3D imaging and navigation systems have also improved the accuracy of the surgery, allowing surgeons to better plan and perform the procedure. These technologies help reduce surgical errors and improve outcomes, ensuring that patients recover faster and with greater success.
Psychological Impact of ACL Surgery
The emotional and psychological impact of ACL surgery is often overlooked. The recovery process can be long and challenging, and many patients experience feelings of frustration, anxiety, or even depression as they navigate their rehabilitation.
Athletes, in particular, may face additional pressures related to the fear of reinjury and returning to their sport. Support from family, friends, and a mental health professional can be incredibly helpful during this time. Some patients benefit from psychological counseling to address these concerns and develop coping strategies.
Maintaining a positive mindset and setting realistic recovery goals is essential to staying motivated throughout the rehabilitation process. Patience and persistence are key to achieving a full recovery and returning to pre-injury levels of activity.
Alternatives to ACL Reconstruction Surgery
Not every ACL tear requires surgery. In some cases, non-surgical treatments can be effective, especially if the tear is partial or the patient does not engage in high-demand activities.
Physical therapy and bracing are the first line of treatment. Strengthening the muscles around the knee can help stabilize the joint, allowing the patient to continue with daily activities without surgery.
In recent years, stem cell therapy and PRP (platelet-rich plasma) injections have been explored as alternatives or adjuncts to surgery. These treatments aim to accelerate healing by promoting tissue regeneration. However, their long-term effectiveness is still being studied, and they are not yet widely used as primary treatments for ACL tears.
For individuals with lower activity demands, non-surgical options may be sufficient to restore function and alleviate pain.
ACL Reconstruction Surgery Costs
The cost of ACL reconstruction surgery can vary significantly depending on several factors, including the patient's location, the surgeon's experience, the type of graft used, and whether the procedure is performed in a hospital or outpatient setting. On average, the cost can range from $5,000 to $20,000 or more.
Insurance typically covers the cost of ACL surgery, especially if the patient is injured while participating in sports or during an accident. However, out-of-pocket expenses may still apply, particularly for high-deductible insurance plans or if the procedure is performed in a facility that does not accept the patient's insurance.
Additionally, rehabilitation costs should be considered, as physical therapy is an essential part of recovery. Many patients will need several months of therapy, which can add another few thousand dollars to the overall cost.
Post-Operative Care for ACL Surgery
Post-operative care is critical for a successful ACL recovery. Immediately after surgery, the knee will be swollen and painful, so elevating the leg, applying ice, and using prescribed pain medications are important. Most patients will use crutches for the first few weeks to avoid putting weight on the knee.
Physical therapy usually begins within the first few days to help reduce swelling and improve range of motion. A progressive rehabilitation plan will focus on strengthening the muscles around the knee to support the new ligament and prevent future injury.
It’s essential to follow all post-surgery instructions to avoid complications and ensure a full recovery.
Long-Term Outlook After ACL Reconstruction
The long-term outlook after ACL reconstruction is generally positive, with most patients able to return to their normal activities or sports within 6 to 12 months. However, full recovery can take time, and some patients may experience lingering discomfort or stiffness.
Patients who follow a comprehensive rehabilitation plan typically regain full function and experience long-term knee stability. However, research indicates that those who return to high-impact sports may be at a higher risk for future knee injuries, including damage to the meniscus or osteoarthritis.
A proper rehabilitation regimen is key to minimizing risks and ensuring the knee remains stable for years to come.
How to Prevent ACL Injuries in the Future
Preventing ACL injuries involves focusing on strength, flexibility, and proper technique. Athletes should engage in exercises that improve the strength of the hamstrings, quadriceps, and other muscles that support the knee joint.
Plyometric and agility training can help athletes improve their ability to pivot, land correctly, and control movement. Proper warm-ups before exercise and using the right footwear also reduce the risk of injury.
Additionally, using knee braces or other protective equipment during high-risk activities can provide extra support for the knee, especially for individuals who have previously injured their ACL.
Conclusion
ACL reconstruction surgery is an effective solution for restoring knee stability and function after a significant tear. The procedure allows many patients to return to active lifestyles and sports. However, it’s essential to consider factors like recovery time, cost, and potential risks before making a decision.
Consulting with a skilled orthopedic surgeon will help you understand whether ACL surgery is the best option based on your individual needs and activity level. With proper surgical technique and a committed rehabilitation plan, ACL reconstruction offers a high success rate and a good long-term outcome for most patients.