Aortic Dissection
What is Aortic Dissection?
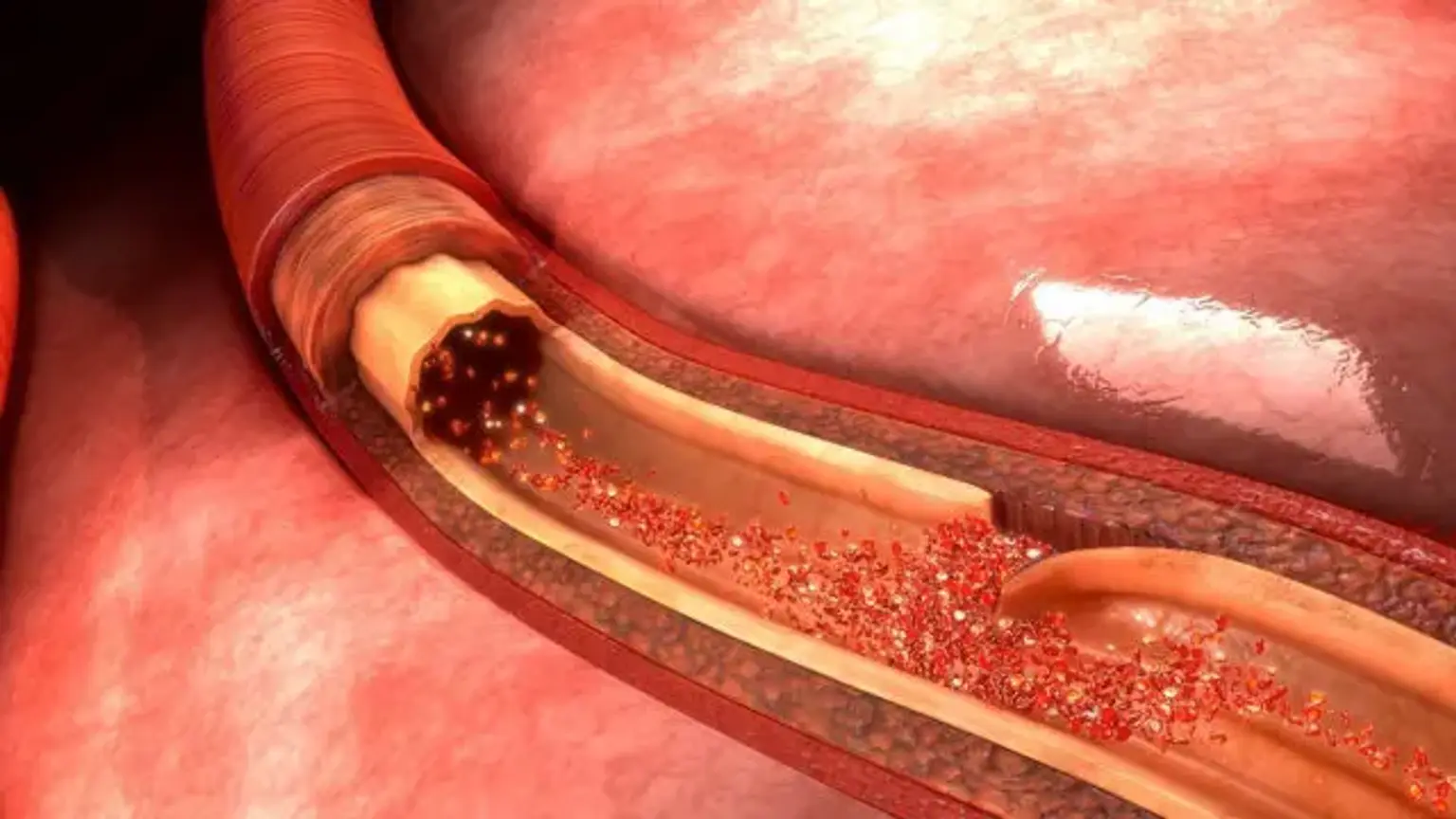
Acute aortic dissection (AAD) is an uncommon but deadly condition. Aorta dissection is caused by the separation of the aortic wall's layers. A rupture in the intimal layer causes the dissection to advance (either proximal or retrogradely), owing to blood penetration between the intima and media. Aortic dissection is linked with a very high mortality rate; the majority of patients die before reaching the emergency department. Patients with a chronic aortic dissection (one that has been present for more than two weeks) had a somewhat better prognosis.
Acute aortic dissection (within 2 weeks) is associated with significant morbidity and death. The first 7 days have the greatest mortality rate; in fact, many patients die before they report to the emergency department (ED) or before a diagnosis is made in the ED. Patients with chronic aortic dissection (lasting more than two weeks) had a better prognosis. Despite advances in diagnostic and treatment techniques, the death rate linked with aortic dissection remains significant.
Anatomy
The aorta is made up of three sections: intima, media, and adventitia. The innermost layer, the intima, is thin and sensitive, lined with endothelium, and readily injured.
The media, which is made up of laminated yet interweaving sheets of elastic tissue, is important for providing strength to the aorta. The spiral arrangement of these sheets gives the aorta its maximum permissible tensile strength. The aortic medium has greater distensibility, elasticity, and tensile strength because it includes relatively little smooth muscle and collagen between the elastic layers. This is in contrast to peripheral arteries, which have more smooth muscle and collagen between the elastic layers.
The adventitia is the aorta's outermost layer. This is mostly made up of collagen. The adventitia contains the vasa vasorum, which feeds blood to the outside portion of the aortic wall. The nervi vascularis, which are bundles of nerve fibers present in the aortic adventitia, is implicated in the creation of pain when the aorta wall is acutely stretched due to dissection. There is no serosal layer in the aorta.
In diastole, the aorta is critical to the forward circulation of blood. The aorta is dilated by blood coming from the left ventricle during left ventricular contraction, and kinetic energy from the ventricle is converted into potential energy stored in the aortic wall. This potential energy is transformed to kinetic energy during aortic wall recoil, moving the blood within the aorta to the peripheral vasculature.
The systolic pressures inside the aorta are determined by the amount of blood expelled into the aorta, the aorta's compliance, and resistance to blood flow. Resistance is mostly caused by the tone of the peripheral arteries, with a little contribution from the inertia produced by the blood column during ventricular systole.
The aorta is divided into two sections: thoracic and abdominal. The ascending, arch and descending segments of the thoracic aorta are separated from the abdominal aorta, which is split into suprarenal and infrarenal segments. The ascending aorta is the anterior tubular section of the thoracic aorta that extends from the aortic root to the innominate artery. The ascending aorta is 5 cm long and consists of an aortic root and an upper tubular section.
The aortic root is made up of the aortic valve, Valsalva sinuses, and left and right coronary arteries. It runs from the aortic valve to the sinotubular junction and supports the aortic leaflets' bases. The aortic root permits the three sinuses of Valsalva to expand outward, allowing the leaflets to fully extend in systole. These sinuses give birth to the left and right coronary arteries.
The aortic arch bends upward between the ascending and descending aortas. The aortic arch gives rise to the brachiocephalic arteries. The aortic arch arteries transport blood to the brain via the left common carotid, innominate, and subclavian arteries.
The aortic arch begins somewhat to the left and in front of the trachea and finishes posteriorly to the left of the trachea and esophagus. The descending aorta runs from the region distal to the left subclavian artery to the 12th intercostal gap. Initially, the descending aorta is located in the posterior mediastinum, to the left of the vertebral column's path.
The abdominal aorta connects the descending aorta from the 12th thoracic vertebra to the bifurcation at the fourth lumbar vertebra. Splanchnic arteries arise from the abdominal aorta. The descending thoracic and abdominal aortas are joined to form the thoracoabdominal aorta.
The elasticity and distensibility of the aorta decrease with age, causing the rise in pulse pressure seen in the elderly. Hypertension, coronary artery disease, and hypercholesterolemia all hasten the course of this process.
Epidemiology
The annual incidence of aortic dissection is estimated to be 5 to 30 incidents per million individuals (compared to the much more common condition of acute myocardial infarction, which affects approximately 4400 cases per 1,000,000 person-years).
In the emergency room, three AADs are eventually diagnosed out of every 1000 patients who arrive with severe back, chest, or stomach pain. Age is a risk factor for nearly 75% of aortic dissections in people aged 40 to 70 years, with the majority occurring between the ages of 50 and 65. There are, nevertheless, some notable distinctions between older adult patients and younger individuals with ascending aortic dissections.
Patients over the age of 65 are far more likely to have atherosclerosis, a previous aortic aneurysm, iatrogenic dissection, or an intramural hematoma. Younger people are far less likely to have a history of hypertension and far more likely to have a connective tissue illness like Marfan syndrome. Furthermore, AAD is three times more prevalent in males than in women, despite the fact that women present later and have worse outcomes.
Aortic dissection types
Presentations are frequently more modest than the classic description of a patient reporting sudden onset of intense 'tearing' chest pain. In as few as 15% to 43% of confirmed AAD patients, physicians properly suspect the diagnosis.
If left untreated, death exceeds 50% during the first 48 hours. Despite a plethora of research, many aortic dissections go undiagnosed in the emergency room.
There are two main anatomic classifications used to classify aortic dissection.
The Stanford system is more commonly used. It divides dissections into two categories based on whether the ascending or descending aorta is affected.
- Type A affects the ascending aorta independent of the location of the main intimal rupture. A type A dissection is one that occurs close to the brachiocephalic artery.
- Type B aortic dissection originating distal to the left subclavian artery and involving only descending aorta.
The DeBakey classification is based upon the site of origin of the dissection.
- Type 1 originates in the ascending aorta and to at least the aortic arch.
- Type 2 originates in and is limited to the ascending aorta.
- Type 3 begins in the descending aorta and extends distally above the diaphragm (type 3a) or below the diaphragm (type 3b).
Ascending aortic dissections are almost twice as common as descending dissections.
Aortic dissection causes
Predisposing high-risk factors for non-traumatic aortic dissection include:
- Hypertension (occurs in 70% of patients with distal Standford type B)
- A sudden, transient, and significant rise in blood pressure (e.g., strenuous weight lifting and use of sympathomimetic agents such as cocaine, ecstasy, or energy drinks)
- Genetic conditions include Marfan syndrome, Ehlers-Danlos syndrome, Turner syndrome, and bicuspid aortic valve, coarctation of the aorta.
- Pre-existing aortic aneurysm
- Atherosclerosis
- Pregnancy and delivery (risk compounded in pregnant women with connective tissue disorders such as Marfan syndrome)
- Family history
- Aortic surgery (coronary artery bypass, aortic or mitral valve replacement, and percutaneous stenting or catheter insertion)
- Inflammatory or infectious diseases that cause vasculitis (syphilis, cocaine use)
Pathophysiology
The aorta wall is divided into three layers: intima, media, and adventitia. Constant exposure to high pulsatile pressure and shear stress weakens the aorta wall, culminating in an intimal tear in vulnerable individuals. Following this rent, blood rushes into the intima-media gap, resulting in the formation of a false lumen.
The majority of these rips occur in the ascending aorta, mainly in the right lateral wall, where the aorta is subjected to the greatest shear strain. An AAD can spread anterogradely and/or retrogradely, causing branch occlusion that results in ischemia of the afflicted region (coronary, cerebral, spinal, or visceral), and proximal type A AADs can induce acute tamponade, aortic regurgitation, or aortic rupture.
The intima covers the genuine lumen in an AAD, whereas the media covers the fake lumen. The genuine lumen is usually less than the fake lumen. Occasionally, the blood flowing through the false lumen causes the formation of an aneurysm with the potential for rupture. The three most prevalent locations for AAD are as follows:
- Nearly 2-2.5 cm above the aortic root (the most common site)
- Just distal to the origin of the left subclavian artery
- In the aortic arch
Aortic Dissection Symptoms
Clinically, the amount of the dissection determines the clinical appearance of AAD, with symptoms correlating to the damaged cardiovascular structures. When conducting history of a patient with suspected AAD, three key factors must be addressed: the quality, radiation, and severity of pain from the outset. Several investigations have shown the severity of pain onset as the most accurate historical component.
While historically reported physical symptoms, such as a disparity in blood pressures in the upper limbs, a pulse deficit, or the presence of a diastolic murmur, increase the chance of AAD when present, they are present in fewer than 50% of confirmed cases of AAD.
Furthermore, the occurrence of chest pain in conjunction with any neurological indication, the combination of chest and abdomen pain, or chest pain followed with limb weakness or paresthesia should raise the clinician's suspicion of AAD.
AAD pain is frequently abrupt, reaches maximum severity rapidly, and can be ripping in nature. The AAD is painless in around 10% of individuals, which is especially frequent with Marfan syndrome. The discomfort may be felt in the front chest if the aorta is ascending, or in the back, if the aorta is descending. As dissection spreads caudally, it may take on a migratory appearance.
One-fifth of patients had neurological abnormalities at the time of presentation. Syncope is another typical symptom that can be caused by hypovolemia, arrhythmias, MI, or elevated vagal tone. If the dissection is antegrade, it may affect the extremities vessels, causing pulse loss, paresthesias, and discomfort.
If the AAD leaks or ruptures in the mediastinum, the patient may have dyspnea and hemoptysis.
Physical findings
Hypertension is particularly prevalent in AAD; if the patient appears with hypotension, this is a serious warning that a rupture has occurred. A blood pressure difference of more than 20mmHg between the arms should raise the possibility of AAD. Among the other features are:
- Wide pulse pressure
- Aortic insufficiency
- Murmur
- Muffled heart sounds (suggesting cardiac tamponade)
- Syncope
- Altered mental status
- Loss of peripheral pulses
Aortic Dissection diagnosis
A high index of suspicion is required for the diagnosis of acute aortic dissection, which entails the following:
- History and physical examination
- Imaging studies
- Electrocardiography
Possible physical examination findings include the following:
- Hypertension
- Hypotension
- Interarm blood pressure differential greater than 20 mm Hg
- Signs of aortic regurgitation (eg, bounding pulses, wide pulse pressure, diastolic murmurs)
- Findings suggestive of cardiac tamponade (eg, muffled heart sounds, hypotension, pulsus paradoxus, jugular venous distention, Kussmaul sign)
- Neurologic deficits (eg, syncope, altered mental status)
- Peripheral paresthesias
- Asymmetrical pulses (eg, carotid, brachial, femoral)
- Progression or development of bruits
Possible laboratory study findings include the following:
- Leukocytosis
- Decreases in hemoglobin values: Leaking or rupture of the dissection
- Elevation of the blood urea nitrogen and creatinine levels: Renal artery involvement or prerenal azotemia
- Elevation of the myocardial muscle creatine kinase isoenzyme, myoglobin, and troponin I and T levels: Myocardial ischemia from coronary artery involvement
- Lactate dehydrogenase elevation: Hemolysis in the false lumen
Routine tests, such as an ECG and a chest x-ray, can assist differentiate between various probable causes of chest discomfort, but they can sometimes be deceptive. In 8% of instances of AAD, ECG abnormalities compatible with an acute myocardial infarction are seen. Furthermore, while a wider aortic profile raises the chance of AAD, its absence does not rule out the diagnosis.
Cardiovascular imaging is required for AAD confirmation to identify the presence of an intimal tear, establish the Stanford classification, and discover valve or branch involvement. For the diagnosis of AAD, most society recommendations prescribe either CT aortography or transesophageal echocardiography (TEE).
The institution's availability and competence should be considered when deciding which modality to use as a first-line screen. Because of its broad availability, CT angiography will most likely be the first sophisticated imaging method used in most emergency departments (EDs).
Blood tests should include a complete blood count (CBC), electrolytes, troponin, D-dimer, and renal function. Smooth muscle myosin heavy chain assay is higher in AAD patients.
A widened mediastinum (>8cm) or fluid accumulation in the hemithorax owing to rupture may be seen on a chest x-ray.
If the patient is stable, a contrast-enhanced CT scan is advised. The spiral CT scan swiftly locate the intimal tear and assist the surgeon in planning the treatment.
Echocardiography
Echocardiography can also be used to detect AAD. Echocardiography is the ideal approach for intraoperative visualization that may be performed at the patient's bedside.
MRI
- The most sensitive method for diagnosing aortic dissection
- Specificity is similar to that of CT
Aortography:
- Has been the diagnostic criterion standard study for aortic dissection
- Is being replaced by newer, safer imaging modalities
Treatment for aortic dissection
Regardless of the site of the dissection, an immediate cardiothoracic or vascular surgical consultation should be undertaken if the diagnosis of AAD is established or strongly suspected. Acute ascending aortic dissections are considered a surgical emergency. For monitoring, the patient should have an arterial line and a central venous catheter. A foley catheter should be placed to measure urine output.
Medical management includes the following:
- Decreasing the blood pressure
- Antihypertensive therapy, beta-blockers, is the treatment of choice for all stable chronic aortic dissections
- Pain management: Narcotics and opiates
Concurrently begin pharmacological therapy, which includes appropriate analgesia (morphine is the chosen analgesic because it inhibits sympathetic output as well) and the administration of short-acting IV beta-blockers aimed at a heart rate of 60 bpm (reductions in heart rate and blood pressure reduces aortic wall tension and limit the extent of dissection).
Non-dihydropyridine calcium channel blockers can be utilized for rate control in patients who are contraindicated to b-blockade. If the systolic blood pressure remains high, nitroprusside can be used to attain a systolic blood pressure target of 100 to 120 mmHg.
Other blood pressure-lowering medications include esmolol, labetalol, and diltiazem. Because they inhibit compensatory tachycardia, B-blockers should be administered with caution in cases of acute aortic regurgitation.
Intravenous fluid injection is an appropriate initial step in hypotensive individuals. Vasopressors can be used to maintain enough perfusion if necessary, however, they may promote additional false lumen propagation. Inotropic drugs should be avoided since they are likely to increase the force and rate of ventricular contraction, causing aortic wall stress to deteriorate.
Aortic dissection surgery
Excision of the intimal rip, obliteration of entrance into the false lumen proximally, and reconstitution of the aorta with the interposition of a synthetic vascular graft are all surgical treatments for type A AAD. Surgical surgery for type B AAD is often reserved for individuals who have a difficult course of the disease.
When AAD involves the ascending aorta, the aorta must be replaced and the valve must be evaluated. Most of the time, the aortic valve must be excised and replaced with a prosthetic valve. Dissections of the descending aorta are complicated and can result in paraplegia. Dissections involving the aortic arch are the most challenging. Surgical mortality ranges from 5 to 20%. Even those who survive must heal over an extended period of time.
Because of the high surgical mortality rate, endovascular treatments are now used to treat AAD. An endovascular stent implantation is associated with much-reduced morbidity as compared to surgery, however, patient selection is critical.
Differential Diagnosis
Alternative diagnoses on the differential of aortic dissection include the following life-threatening conditions:
- Myocardial infarction,
- Aortic aneurysm,
- Cardiac tamponade
- Esophageal rupture (Boerhaave syndrome),
- Spontaneous pneumothorax,
- Pulmonary embolism, and
- Stroke / transient ischemic attack.
If a patient has abdominal pain, renal or biliary colic, bowel obstruction/perforation, or intestinal obstruction/perforation, non-dissection-related mesenteric ischemia should be examined. Non-dissection-related embolic events or arterial blockage can cause pulse deficit.
Prognosis
Aortic dissection still has a significant death rate. At least 30% of patients die after arriving at the emergency room, while death rates following surgery range from 20% to 30%. Comorbidity puts a toll on individuals who survive the procedure, and their quality of life suffers as a result. The first 10 days after an acute aortic dissection had the highest death rate. Patients with chronic dissection have a better prognosis, although their life expectancy is reduced when compared to the general population.
Several studies have found that when patients are handled by an interprofessional team of healthcare specialists that includes a cardiologist, intensivist, pulmonologist, nephrologist, cardiac surgeon, interventional radiologist, and anesthesiologist, their results increase.
Furthermore, the pharmacist must educate the patient on the significance of blood pressure control and drug adherence. Aortic dissection results seem to be better at big volume centers compared to small centers that conduct fewer than 5 cases per year.
Complications
- Multiorgan failure
- Stroke
- MI
- Paraplegia
- Renal failure
- Amputation of extremities
- Bowel ischemia
- Tamponade
- Acute aortic regurgitation
- Compression of superior vena cava
- Death
Conclusion
If undetected, aortic dissection is a medical emergency with a very high fatality rate. Because the majority of patients arrive to the emergency department, an interprofessional team is essential.
When a patient with an aortic dissection arrives at the emergency room, a standardized protocol must be in place to guarantee that the diagnosis and care are completed as soon as possible. The triage nurse should be well informed of the significance of the patient's rapid admittance and confer with the emergency physician and heart surgeon.
The technique of diagnosis is determined by the patient's stability and the availability of imaging testing. An ECHO or a CT scan are the two alternatives. A patient who is unstable should never be sent to the radiology suite. A cardiologist should be sought instead for a bedside echo.