Coronary Artery Bypass Graft (CABG)
Overview
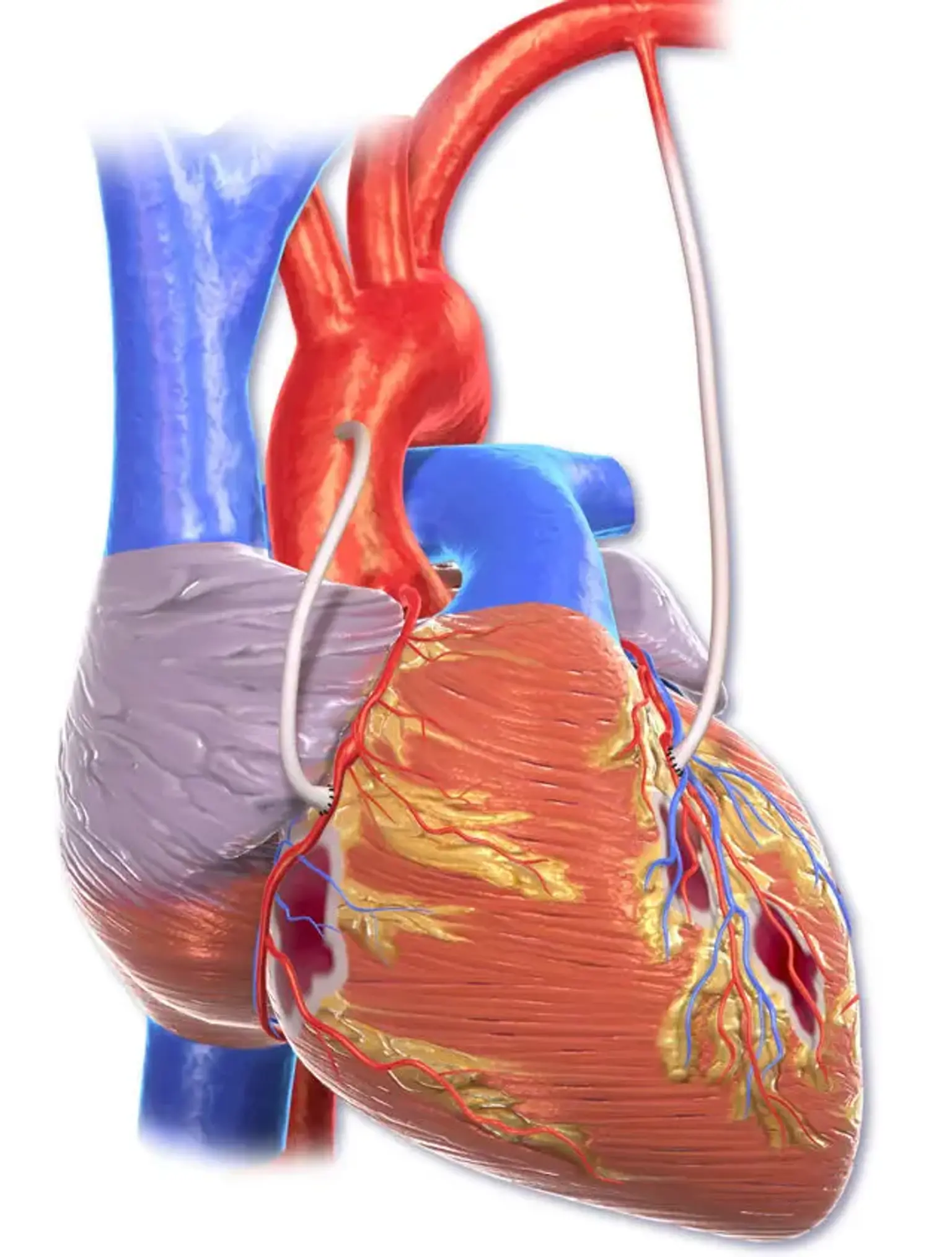
CABG is a significant surgical procedure in which atheromatous obstructions in a patient's coronary arteries are bypassed using harvested venous or arterial conduits. The bypass restores blood flow to the ischemic myocardium, restoring function and viability and alleviating anginal symptoms.
Almost 400,000 CABG operations are conducted each year, making it the most regularly performed major surgical surgery; however, surgical trends have shifted as alternate choices such as medical therapy and percutaneous coronary intervention (PCI) have become more popular.
CABG surgery
Coronary artery bypass grafting (CABG) is a procedure used to enhance quality of life and minimize cardiac-related mortality in individuals with coronary artery disease (CAD). CAD is the biggest cause of death in the United States and the industrialized world, affecting 16.5 million US adults (aged 20 years) each year.
It is responsible for 530,989 fatalities in the United States each year, and the long-term consequences of CAD, including as left ventricular dysfunction and heart failure, are expected to impact nearly 8 million persons over the age of 18 by 2030.
CABG surgery was first performed in the 1960s with the goal of providing symptomatic alleviation, improved quality of life, and enhanced life expectancy to CAD patients. When compared to medical treatment, CABG increased survival rates in individuals with multivessel disease and left main disease by the 1970s.
The new CAD treatment paradigm asks for a heart team approach in which the cardiologist and the cardiac surgeon evaluate the coronary angiography together and provide the patient the best available alternative for coronary revascularization, whether it be implantation of a percutaneous coronary stent or CABG. At the moment, the average CABG patient is older, has had prior percutaneous coronary intervention (PCI), and has much more comorbidities.
Despite these risks, CABG remains one of the most important surgical operations in modern medicine history, having probably saved more lives and offered more considerable symptomatic relief than any other major surgery. New minimally invasive approaches, breakthroughs in anesthesia and intensive care unit (ICU) management, and technology advancements are pushing the limits of this operation to new heights.
In general, there are two types of CABG surgical procedures: on-pump and off-pump, with the difference being that an on-pump CABG uses a cardiopulmonary bypass circuit and an arrested heart to work. The left internal mammary artery (LIMA) and saphenous vein grafts (SVG) from the lower extremities are commonly employed as bypass graft conduits.
The right internal mammary artery (RIMA), the radial artery, and the gastroepiploic artery are some of the other conduits that can be transplanted. The kind and position of the grafts are determined by the patient's anatomy and the location of the blocked arteries. The LIMA is typically grafted to the left anterior descending (LAD) artery, while the other conduits are utilized to access the other blocked arteries.
Anatomy and Physiology
Two major coronary arteries supply the myocardium of the heart: the left main coronary artery and the right coronary artery (RCA). The left main coronary artery is typically a short section that divides into the left anterior descending (LAD) and circumflex arteries. The LAD divides into diagonal branches, whereas the circumflex artery divides into obtuse marginal branches. The RCA divides into two branches: the posterior descending artery (PDA) and the marginal branches.
Depending on which artery supplies the interventricular septum and PDA, the coronary circulation can be categorized into left-dominant, right-dominant, and co-dominant systems. The circumflex artery supplies the PDA in a left-dominant system, whereas the RCA supplies the PDA in a right-dominant system. With co-dominant vascular supply, the PDA is fed by both the RCA and the circumflex arteries at the same time.
Blockages in any of the coronary arteries result in a corresponding deficiency in myocardial perfusion, ischemia, and if left untreated can result in a permanent infarction or damage to the heart.
Historical information
In 1912, Alexis Carrel was awarded the Nobel Prize in Physiology and Medicine for his work. His knowledge of the relationship between angina pectoris and coronary artery stenosis enabled him to anastomose a carotid artery segment from the descending thoracic aorta to the left coronary artery in a canine model.
Arthur Vineberg, a notable Canadian surgeon, transplanted the left internal thoracic (mammary) artery directly into the myocardium of the anterior left ventricle in patients with severe angina pectoralis in the late 1940s. Surprisingly, a few individuals had considerable symptom reduction as a result of this surgery.
Sabiston conducted the first planned saphenous vein bypass procedure for coronary revascularization at Duke University in 1962. Kolessov utilized the left internal thoracic (mammary) artery to bypass the left anterior descending artery without cardiopulmonary bypass in 1964, and Carpentier pioneered the use of radial artery grafts as CABG conduits in 1973.
CABG flourished as the sole treatment for CAD throughout the 1970s and early 1980s. The number of CABG surgeries done decreased with the development, introduction, and widespread adoption of percutaneous coronary artery stenting in the 1980s and 1990s. Several multicenter trials comparing CABG to current stent treatment, however, have clearly established the advantages of CABG, particularly when specific patient features such as diabetes, multivessel CAD, and ischemic cardiomyopathy are included.
Indications for CABG
When there are high-grade blockages in either of the main coronary arteries and/or percutaneous coronary intervention (PCI) has failed to eliminate the blockages, CABG is often advised. The following are the Class 1 recommendations from the 2011 ACCF/AHA guidelines:
- Left main disease greater than 50%
- Three-vessel coronary artery disease of greater than 70% with or without proximal LAD involvement
- Two-vessel disease: LAD plus one other major artery
- A severe stenosis of more than 70% in a patient with considerable anginal symptoms despite maximum medication treatment
- In a survivor of sudden cardiac death with ischemia-related ventricular tachycardia, one vascular disease was more than 70%.
Other indications for CABG include the following:
- Disabling angina (Class I)
- Ischemia that persists in the context of a non-ST segment elevation myocardial infarction (NSTEMI) that is refractory to medicinal treatment (Class I)
- Poor left ventricular function, but viable, nonfunctioning myocardium above the anatomic defect that can be revascularized.
- Clinically severe CAD with 70 percent or higher stenosis in one or more vessels, as well as refractory angina despite medication treatment and PCI
- Clinically severe CAD of 70% or more stenosis in 1 or more vessels in survivors of sudden cardiac arrest thought to be caused by ischemic ventricular arrhythmia
- Clinically severe CAD with 50% or more stenosis in 1 or more vessels in patients undergoing cardiac surgery for other reasons (eg, valve replacement or aortic surgery)
CABG may be performed as an emergency treatment in the setting of an ST-segment elevation MI (STEMI) if percutaneous coronary intervention (PCI) was not possible or if PCI failed and there is prolonged pain and ischemia affecting a major portion of myocardial despite medicinal therapy.
Factors that increase the survival benefit of CABG include the following:
- Left ventricular ejection fraction of 45% or less
- Diabetes mellitus
- Ischemic mitral regurgitation
- PCI failure, with or without acute MI (AMI)
Contraindications
CABG is not recommended for asymptomatic individuals who are at low risk of MI or death. Patients who will benefit little from coronary revascularization are likewise excluded.
Although senior age is not a contraindication, CABG should be approached with caution in the elderly, particularly those over the age of 85. These individuals are also more prone to have perioperative problems following CABG. In patients with complicated CAD, a multidisciplinary cardiac team approach emphasizing shared decision making is critical to provide the patient with the best chance of a successful revascularization plan.
CABG procedure
In addition to the coronary angiography that detected the coronary artery disease, the patient will require various tests conducted in preparation for surgery. Laboratory tests such as a complete blood count (CBC), metabolic panels including liver function tests, coagulation panels, and hemoglobin A1c will be required. Other tests, including as an electrocardiogram (ECG), echocardiography, carotid ultrasonography, chest x-ray, and maybe a CT chest or vein mapping of the lower limbs, may be necessary.
To avoid arrhythmias such as atrial fibrillation, preoperative medicines such as beta-blockers are frequently given during the perioperative period. Previously, aspirin was withheld 5 to 7 days before surgery, but it is now suggested to begin or continue preoperatively.
When the patient arrives at the hospital, intravenous access will be established, and their medicines and preoperative tests will be examined. Hair will be removed from the surgery locations, and the patient will be given a chlorhexidine bath.
Equipment
This significant surgical surgery necessitates not just the equipment required for most other surgical operations, but also several specialized pieces of equipment, such as a cardiopulmonary bypass machine with a heater-cooler device to warm and cool the blood.
Personnel
The operation is performed by a specialized cardiovascular surgical team with extensive training and experience with taking care of these complex patients. The team consists of the cardiothoracic surgeon and their assistants, anesthesiologists, nurses, surgical technicians, and perfusionists
Assessment of Risk
Risk models for predicting 30-day mortality after isolated CABG are being developed. The most often used predictors in cardiac surgery are the Euroscore system and the Society of Thoracic Surgeons (STS) 2008 Cardiac Surgery Risk Model. Age, prior MI, PVD, renal failure, hemodynamic status, and EF are all shared factors in these two outstanding models. Eight of the most relevant factors, including age, surgical acuity, reoperative status, creatinine level, dialysis, shock, chronic lung disease, and EF, explain 78 percent of the variation in the STS model.
Premedication
Premedication seeks to reduce myocardial oxygen needs by lowering heart rate and systemic arterial pressure, as well as to increase myocardial blood flow using vasodilators. The following medications should be taken up to the time of surgery:
- Beta-blockers, calcium channel blockers, and nitrates
- Aspirin
Administered agents are as follows:
- Temazepam immediately preoperatively
- Midazolam, a small intravenous (IV) dose in the operating room before arterial line insertion
Each patient should get 2 units of blood (for mild cases) or 6 units of blood, fresh frozen plasma, and platelets cross-matched (for complex cases). Tranexamic acid (1-g bolus before surgical incision, followed by a 400 mg/hr infusion during surgery) may be considered to minimize postoperative mediastinal hemorrhage and the amount of blood products necessary (ie, red blood cell and fresh frozen plasma)
Anesthesia
Cardiac surgery is most usually conducted under deep general anesthesia with endotracheal tube. The following two types of neuraxial blockade are used seldom as adjuncts:
- Intrathecal opioid infusion
- Thoracic epidural anesthesia (generally a low-dose local anesthetic/opioid infusion)
Technique
The process begins after the patient is in the operating room and is connected to standard monitors. Before inducing general anesthesia, an anesthesiologist may insert an arterial line to monitor the patient's blood pressure invasively. Following the induction of general anesthesia and intubation of the patient, a central line for venous access and a pulmonary artery catheter may be inserted, followed by the insertion of a transesophageal echocardiography transducer.
Before the surgical incision, the patient is sterilely prepared and draped, and a time-out is administered. The surgeon performs a medial sternotomy to prepare for the removal of the LIMA for use as a conduit. A trained assistant, generally a physician assistant, nurse first assistant, or another surgeon, uses open or video-assisted procedures to remove the saphenous vein from one or both legs at the same time.
Following the acquisition of adequate conduits, the surgeon prescribes anticoagulation, most often heparin, to be administered in preparation for cardiopulmonary bypass (CPB). The aorta and heart of the patient are centrally cannulated, and tubing is connected to the cardiopulmonary bypass circuit. Following the initiation of CPB, the heart is stopped with high-potassium cardioplegia so that the surgeon can anastomose the harvested conduits to the coronary arteries distant to the obstructions.
As conduits for coronary artery bypass grafting, either arteries or veins can be employed (CABG). A key publication from the Cleveland Clinic proved the survival advantages of grafting the left internal thoracic (mammary) artery to the left anterior descending coronary artery many years ago. This is still true; in fact, if possible, bilateral internal thoracic (mammary) artery grafting offers a considerable long-term survival benefit. Strong evidence shows that using an extra artery graft rather than a venous graft is related with improved long-term results.
The larger saphenous vein and, on rare occasions, the short saphenous vein are the most regularly used vein grafts, whereas the internal thoracic (mammary) artery is the most usually utilized artery transplant. The radial artery graft was reintroduced into clinical practice in the 1990s and continues to demonstrate high patency rates of 80% or more after 10 years follow-up, particularly if the target vascular stenosis was greater than 90%.
The downside of saphenous vein grafts is that their patency declines with time: 10-20% are blocked 1 year after surgery due to technical mistakes, thrombosis, and intimal hyperplasia. Another 1-2 percent of vein grafts occlude every year from 1 to 5 years following surgery, and another 4-5 percent occlude every year from 6 to 10 years. Vein graft occlusion that occurs one or more years after CABG is caused by vein graft atherosclerosis, which is accompanied by the development of neointimal hyperplasia.
Only 50-60% of saphenous vein grafts are patent 10 years following surgery, and only half of them are free of angiographic atherosclerosis. Patients should take life-long antiplatelet medication, most typically in the form of daily low-dose (81 mg) aspirin, as part of proper secondary prophylaxis.
Internal thoracic (mammary) artery grafts, unlike saphenous vein grafts, maintain patency throughout time. More than 90% of internal thoracic (mammary) artery grafts are still patent after 10 years. When the left anterior coronary artery is bypassed, the left internal thoracic (mammary) artery should be utilized as the conduit.
The conduits are linked to new ostia generated in the proximal aorta after the surgeon anastomoses the distal parts. The cardioplegia is then rinsed away, the heart begins to contract, and the surgeon may examine the grafts for blood flow and competency, as well as bleeding from the anastomosis sites. The chest is then closed with sternal wires, and the patient is moved to the critical care unit for hemodynamic stability monitoring and extubation.
Complications
Stroke, wound infection, graft failure, renal failure, postoperative atrial fibrillation, and mortality are all possible consequences of CABG. The stroke rate after CABG has been reported to range between 1% and 2%, depending on the patient's features and risk factors for stroke, which include advanced age, previous stroke, aortic atherosclerosis, peripheral artery disease, perioperative atrial fibrillation, and diabetes.
Sternal wound infection rates are around 1% and are affected by risk variables such as obesity, diabetes, chronic obstructive pulmonary disease (COPD), and operation length.
Failure of a saphenous vein graft (SVG) is most likely within 30 days after surgery and is caused by numerous reasons such as vein size and excessive length, distal runoff and poor flow, and hypercoagulability and thrombosis. With repeat angiography following CABG, rates of SVG failure as high as 25% have been seen. Alternatively, arterial grafts like the left internal mammary artery (LIMA) and radial arterial grafts last longer and have patency rates that reach 90% after 10 years.
Postoperative renal failure rates following CABG vary from 2% to 3%, with 1% needing dialysis. Preoperative renal illness, old age, diabetes, type of surgery, LV dysfunction, and shock are all risk factors. Although no drugs have been definitely proved to diminish the rates of CABG-induced renal impairment, off-pump CABG may offer a benefit over on-pump CABG.
Atrial fibrillation within the first 5 days following CABG is rather frequent, with rates ranging from 20% to 50%, and is linked with increased morbidity, including a greater risk of embolic stroke and death. The most effective strategy to minimize the incidence of postoperative atrial fibrillation has been proven to be preoperative therapy with beta-blockers and perhaps amiodarone.
The risk of perioperative mortality following CABG varies according to co-morbidities, the urgency of the surgery, and the case-volume of the facility where the procedure is performed, ranging from 1% to 2%.
Outcomes
According to a meta-analysis of six randomized clinical trials involving 6055 patients from the era of arterial grafting and stenting, coronary artery bypass grafting (CABG) leads to a reduction in long-term mortality and myocardial infarctions (MIs) as well as reductions in repeat revascularizations in patients with multivessel coronary disease, regardless of whether patients are diabetic or not.
A meta-analysis of eight randomized trials involving 3612 adult patients with diabetes and multivessel coronary artery disease (CAD) found that CABG lowered the risk of all-cause death by 33% after 5 years when compared to PCI. When patients who had CABG were compared to subgroups of patients who got either bare metal stents or drug-eluting stents, the relative risk decrease did not vary substantially.
Patients aged 51 to 70 years and those older than 70 years who received CABG within the same time period fared considerably worse in terms of survival. Chronic renal disease, a low left ventricular ejection fraction, peripheral vascular disease, or chronic obstructive pulmonary disease were the leading risk factors for all-cause death.
The Surgical Treatment for Ischemic Heart Failure (STICH) Extension Study (STICHES) concluded that the rates of death from any cause, death from cardiovascular causes, and death from any cause or hospitalization for cardiovascular causes were significantly lower in patients who underwent CABG and received medicare.
Furthermore, there was a considerable hospital-level variance in STEMI CABG rates, and CABG was frequently done within 1-3 days of angiography. Patients who received CABG and those who did not had similar in-hospital death rates.
A meta-analysis of 6637 patients with unprotected left main CAD from nine trials over a 14-year period (2003-2016) found that PCI with drug-eluting stents was associated with comparable cardiac and all-cause mortality but reduced rates of stroke and greater rates of repeat revascularization. For significant adverse cardiac and cerebrovascular events, a trend favoring CABG vs PCI did not achieve statistical significance.
In terms of quality of life after CABG versus PCI for multivessel CAD, both procedures improve the frequency of angina. However, at 1 month postprocedure, PCI patients tend to recover quicker and have better short-term health status than CABG patients, however at 6 months and longer postprocedure, CABG patients appear to have better angina alleviation and quality of life than PCI patients.
Conclusion
A coronary artery bypass graft (CABG) is a surgical technique used to treat coronary heart disease with the goal of improving quality of life and lowering cardiac-related mortality. It redirects blood around constricted or obstructed sections of the main arteries, increasing blood flow and oxygen delivery to the heart.