Carotid Artery Stenting
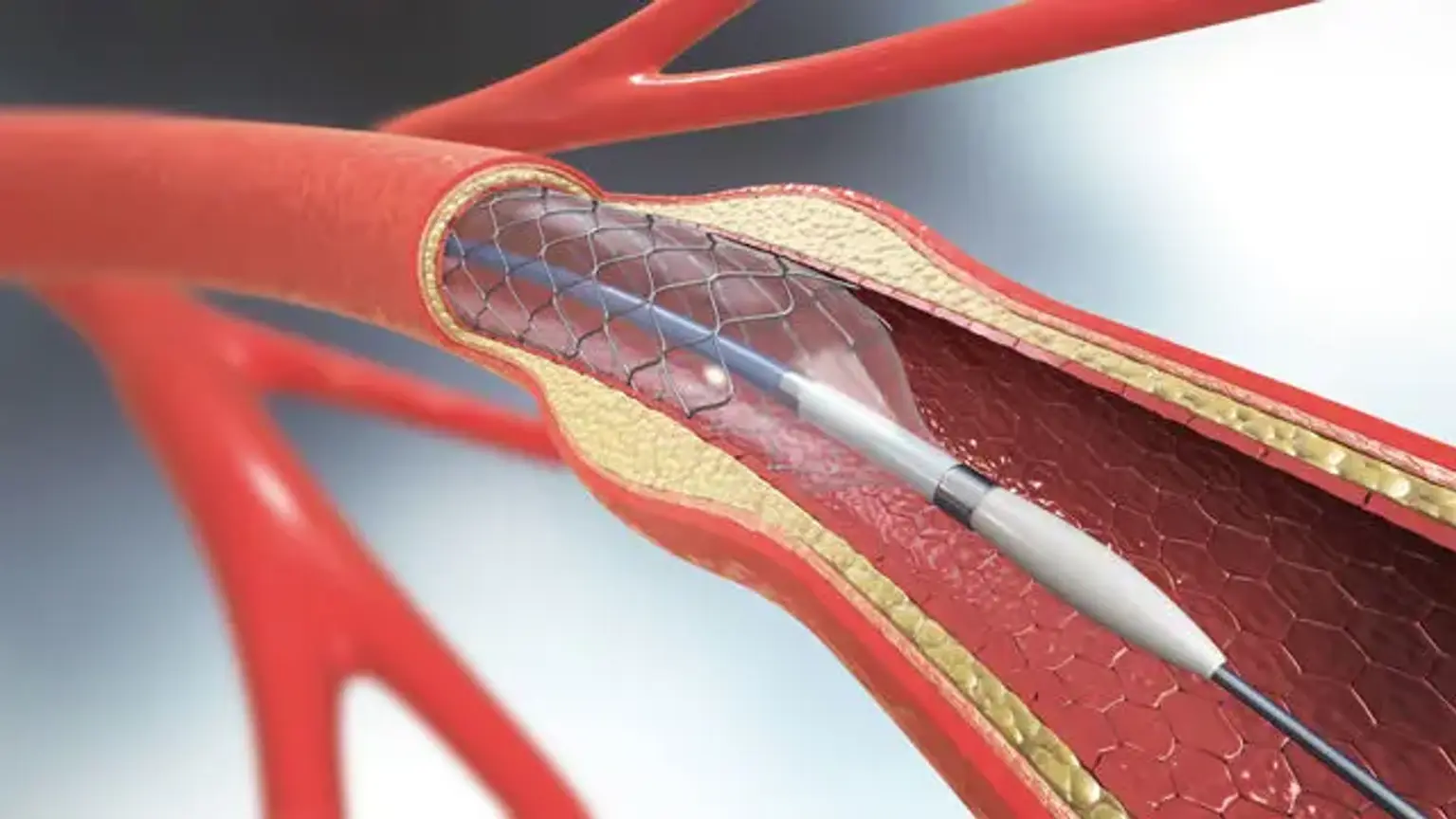
Traditional treatment for high-grade asymptomatic and symptomatic carotid artery stenosis has been carotid endarterectomy (CEA). Carotid endarterectomy is a procedure that involves exposing the carotid artery and removing plaque from the carotid bulb and internal carotid artery through a neck cut. Minimally invasive procedures have progressed in vascular surgery, as they have in many other surgical fields throughout time. Smaller cuts, less postoperative discomfort, a lower risk of postoperative wound problems, and a shorter hospital stay are all advantages of these procedures. One such procedure is carotid artery stenting (CAS), which can be done via a transfemoral or transcarotid route.
Anatomy and Physiology
The aortic arch (left) or the brachiocephalic trunk (right) give rise to the common carotid artery. It is divided into two carotid arteries: internal and external carotid. The external carotid artery supplies blood to the face, scalp, and neck, whereas the internal carotid artery supplies blood to the brain. At various points, the internal and external carotid arteries develop collaterals. In the event that either artery becomes clogged, this is useful for maintaining blood flow through collateral circulation. There are three distinct anatomic forms of the aortic arch. To make things easier, an imagined horizontal line is marked through the top of the aortic arch and imagined parallel lines are made to compare the origins of the great vessels emerging off the arch. All great vessels begin near the imaginary horizontal line drawn through the top of the aortic arch in a type 1 arch. A type 2 aortic arch is defined by the origins of all major vessels falling within the second parallel line. The sources of all major vessels lie within the third parallel line for a type 3 aortic arch. The angulation of the aortic arch, as it relates to the type of aortic arch, has a significant impact on CAS.
Coronary Artery Stenting Indications
In individuals with high-grade asymptomatic (greater than 75%) or symptomatic carotid artery stenosis, CAS is a viable option to CEA. High surgical patient risk, such as serious pulmonary disease, current myocardial infarction, unstable angina, or severe congestive heart failure; a history of previous neck radiation that is expected to make open surgical dissection challenging; the presence of a tracheostomy, contralateral carotid obstruction; and prior CEA with reoccurring stenosis are all indications for CAS.
Coronary Artery Stenting Contraindications
The unfavorable aortic arch structure is the primary contraindication to CAS via a transfemoral route. A severely calcified aortic arch or a type 3 aortic arch are examples of this. History of life-threatening allergic reaction to intravenous contrast dye can be a relative contraindication. Patients can, however, be pre-medicated to reduce some of the hazards. A common carotid artery length of less than 5 cm from the clavicle is deemed unsuitable for a transcarotid approach.
Equipment
Both procedures require an ultrasound scan, fluoroscopic imaging equipment, lead shielding, sterile drapes, anticoagulated saline, and heparin. To confirm that the ACT following heparinization is greater than 250 seconds, an ACT machine should be available.
The following items are required for the transfemoral approach:
- Micro-puncture kit for percutaneous access of the common femoral artery
- Various sizes wires
- 6 French short and long sheaths
- Angled catheters
- Angioplasty balloons
- Embolic protection device
The transcarotid technique necessitates the following:
- An operating table
- Vascular clamps for the surgical exposition of the common carotid artery at the base of the neck and direct puncture with a micro-puncture kit,
- Additional wires, sheaths, and balloons may be employed.
- A flow reversal device that protects the brain from embolization.
Coronary Artery Stenting Preparation
Most clinicians choose to conduct CAS under local anesthetic with or without sedation in the case of a transfemoral approach to evaluate the patient's neurologic condition. Local anesthesia with sedation or general anesthesia may be used for the transcarotid approach. The use of intraoperative EEG/brain mapping should be recommended if general anesthesia is used.
Patients should be thoroughly observed throughout the procedure, regardless of the method used. CAS, like CEA, can induce significant alterations in a patient's hemodynamics, such as hypotension or bradycardia. To manage such hemodynamically substantial alterations, anesthesia practitioners should have vasoactive drugs on hand. Having an arterial line in situ for invasive hemodynamic monitoring during the operation is also a good idea. Patients should take aspirin and Plavix before surgery, and they should continue to take them afterward. In the preoperative holding room, all patients should be questioned about their use of aspirin and Plavix.
The patient should be supine and the neck should be shifted to the other side for the transfemoral approach. The patient should be supine with a shoulder roll underneath the shoulders and the neck moved to the opposite side for the transcarotid approach. As with any invasive surgery, complete sterile precautions should be followed during the procedure. Both groins should be cleaned and draped in the usual sterile manner if the transfemoral technique is employed.
In addition to the groins, the neck should be prepared and draped for the transcarotid approach.
Coronary Artery Stenting Procedure
Transfemoral Carotid Artery Stenting
The transfemoral method is thought to provide greater versatility. However, aortic arch structure and calcifications can limit it. The common femoral artery is percutaneously reached using a micro-puncture kit and the Seldinger technique under ultrasound guidance. A femoral angiography is recommended at this point to determine correct anatomic entrance into the common femoral artery and determine suitability for use of a vascular access closure device after the procedure's completion. Following that, a 6 Fr sheath is applied over a 0.035 inches wire. The wire is carefully inserted into the aortic arch. The common carotid artery is preferentially cannulated and mapped using an angled catheter and a left anterior oblique projection on the fluoroscopic system. The catheter is then put into the external carotid artery once the guidewire has been inserted into the artery. A shuttle sheath is introduced into the common carotid artery over a stronger wire. To locate the lesion, specialized carotid arteriograms are conducted from various perspectives. After traversing the lesion with a 0.014 inches wire, an embolic protection device should be placed. A small profile balloon is used to dilate the lesion before surgery. During this procedure and afterward, pay close attention to the patient's hemodynamics. A properly sized stent is inserted after pre-dilation. If there is severe residual stenosis (more than 35%) after the stent is deployed, balloon angioplasty can be used to correct it. If the results are favorable, the carotid and cerebral angiograms are completed, and the catheters and sheaths are removed. The arteriotomy site in the common femoral artery is then closed with a closure device.
Transcarotid Carotid Artery Stenting
The transcarotid method includes surgically exposing the common carotid artery at the base of the neck. In addition to typical anatomic landmarks, duplex ultrasonography can be utilized to design the surgical incision throughout the course of the common carotid artery. Bovie electrocautery is used to carry out the dissection via the subcutaneous tissues. The platysma is separated and identified. The common carotid artery is then discovered and circumferentially dissected. The artery is subsequently enveloped in a vascular loop or umbilical tape. The proximal and distal portions of the common carotid artery are also torn out. The common carotid artery is directly accessible using a micro-puncture kit, and angiography is obtained. The arterial portion of the flow reversal device is then inserted across the guidewire in the common carotid artery. The common femoral vein is pierced using a micro-puncture kit under ultrasound supervision, and a 0.035 guidewire is then introduced into the femoral vein, followed by implantation of the flow reversal system's venous sheath. The venous sheath is subsequently connected to the arterial sheath, resulting in reverse flow. Multiple projections of carotid angiography are then conducted. After traversing the lesion with a guidewire, a clamp is placed over the proximal common carotid artery. To address the carotid artery lesion, pre-dilation and stent placement are conducted after this maneuver. Balloon angioplasty is used to treat significant residual stenosis following stent deployment (usually greater than 35%). The wires and catheters are withdrawn after the angiography is finished. The distal common carotid artery is clamped, and the arteriotomy is suture-mediated closed with proline suture. The incision in the neck is closed in layers. The femoral vein sheath is withdrawn, and manual pressure is applied to achieve hemostasis.
What is the Recovery Time for Carotid Artery Stenting?
After carotid stent placement, most people stay in the hospital for 24 to 48 hours. The hospital personnel will keep an eye on your vital signs during this period to make sure you are okay. An ultrasound examination may also be performed to ensure that the artery is clear.
Nurses will monitor your vital signs throughout the night to ensure that you recover quickly. If no problems are discovered within 24 hours, you will most likely be discharged from the hospital. Patients may be monitored for an additional day or two in some circumstances.
The majority of the carotid stent recovery will occur at home. Most people should rest for at least 48 hours and avoid engaging in vigorous activity.
Over the next few days, you may have pain at the wound site. This is a common occurrence during the recovery period. To alleviate the discomfort, the doctor may prescribe a painkiller. However, many individuals find that acetaminophen provides the relief they desire. If the discomfort persists for longer than three days, you should seek medical advice.
You can resume your normal routine after a day to three. It is still a good idea to stay away from strenuous activities for around 6 to 7 days, or until the wound site is completely healed. Instead, go for brief walks to keep the heart and circulatory system in good condition. After a week of recovery, you should be capable of exercising yourself more.
Coronary Artery Stenting Risks
- Hemodynamic instability. baroreceptors in the carotid bulb regulate sympathetic and parasympathetic functions. With angioplasty and stent installation, these receptors are stretched/compressed, which inhibits sympathetic activity and increases vagal parasympathetic tone, resulting in cardiovascular disturbances. Although bradycardia and hypotension can occur in five to ten percent of patients, routine preprocedural steps such as avoiding beta-blockers close to intervention time and prescribing atropine with a low heart rate baseline (less than 60 beats per minute) can help to minimize substantial hemodynamic changes. Although the majority of these alterations are transient and may not necessitate long-term treatment, some people may receive short-term vasopressor treatment. Doctors choose IV dopamine because it is a vasopressor with inotropic characteristics that enhances renal and hepato-splanchnic blood flow and raises cardiac output more than norepinephrine.
- Iatrogenic vascular injury. Vasospasm is typically benign, short-lived, and only noticeable in 12-15% of instances due to iatrogenic vascular injury. Vascular dissections, thrombosis, or perforation, on the other side, are more dangerous and can serve as a nidus for thrombosis; nonetheless, they are less frequent.
- External carotid artery stenosis. it can occur as a result of the ICA straightening and dilatation caused by the stent placement, however, it is regarded clinically inconsequential.
- Device malfunctioning. Device failure is uncommon, occurring in fewer than 1% of cases, and can include stent migration, twisting, or fracture, which can result in vascular angulation and restenosis.
- Stent restenosis or thrombosis. Restenosis or thrombosis of a stent might lead to hypoperfusion and thromboembolism. Intimal hyperplasia is a post-angioplasty and stenting healing consequence of the vascular intervention. The extracellular matrix and vascular smooth muscles are usually affected, resulting in enlargement of the intimal vessel wall layer. Excessive intimal hyperplasia might restrict luminal blood flow, resulting in restenosis within the stent. Greater stent length, stent radius, multi-vessel involvement, residual underlying dissection as well as poor apposition to the vessel wall, advanced age, female sex, elevated Systolic and diastolic blood pressure, previous or active tobacco use, non-insulin-dependent diabetes, high serum cholesterol, and higher-grade contralateral carotid stenosis are among the technical and demographic factors linked to this. A recent randomized trial found that using cilostazol to prevent in-stent carotid stenosis had encouraging results.
- Cerebral hyperperfusion syndrome. individuals with impaired vasomotor responsiveness at baseline and periprocedural times, as well as untreated hypertension and obstructed or severe contralateral carotid stenosis, are at a greater risk of postprocedural intracranial hemorrhage. Patients at the greatest risk for cerebral hyper-perfusion syndrome may be identified with pre-procedure testing to determine the presence of a damaged cerebrovascular reserve. Transcranial Doppler with measurement of mean flow middle cerebral artery velocities before and after revascularization can be utilized to titrate postoperative blood pressure levels.
- Myocardial infarction. Periprocedural myocardial infarction is estimated to comprise 2-4% of all myocardial infarctions. In addition to chest discomfort or ECG evidence of ischemia, myocardial infarction is characterized by a doubling of the upper limits of the normal range of creatine kinase MB or troponin. Hemodynamic imbalance during angioplasty/stenting is thought to be the primary cause of myocardial ischemia.
- Access site problems. transfemoral access injuries are the most common consequences. Pain is the most common problem, but infections, pseudoaneurysms or arteriovenous fistulas, puncture-site hematoma, and retroperitoneal hemorrhage necessitating blood transfusion are less common. Transradial artery access for neuroendovascular treatments, such as carotid stenting, is becoming more common, and it may be safer than transfemoral access.
Clinical Significance
CAS and CEA have been compared in both symptomatic and asymptomatic patients in a number of studies. CEA tends to increase the chance of myocardial ischemia, whereas CAS appears to increase the risk of a cerebrovascular accident (CVA). After two years, the rates of restenosis appear to be comparable between CEA and CAS. Patients aged 70 and up, as well as those with a significant burden of white-matter lesions on brain scans, seem to have worse results with CAS as a technique. As a result, patient selection is critical in CAS. In the event of a hostile aortic arch, the transcarotid approach of CAS may lessen the risk of embolization. In ongoing studies, more experience with this method is being obtained. CEA- and CAS-related hospitalization and long-term expenses seem identical.
Coronary Artery Stenting Future Directions
Carotid stenting, despite being a well-established method with great results when performed by experienced operators in high-volume centers, is struggling to gain scientific acceptance. The undeniable discrepancy in outcomes between the two techniques shown in randomized clinical studies has dampened initial enthusiasm for CAS as a viable and less invasive substitute to CEA. Inadequate endovascular expertise requirements, which could contribute to an elevated event rate due to both insufficient technical abilities and poor patient selection, have been identified as the primary cause of unfavorable CAS results. Despite the fact that high-quality multi-center registries and high-volume single-center experiences have repeatedly indicated favorable CAS results, the neurologist community has not deemed the data enough to prescribe CAS. Furthermore, the surgery has only been funded within study procedures in several countries, including the United States. In recent years, the number of surgeries performed has remained stable, if not declining, while corporate investment for research, development, and clinical studies has been drastically reduced. Unfortunately, little new randomized data comparing CAS with CEA is expected in the next years. Only if the promising technologies described are given the opportunity to be tested in appropriately powered clinical studies, which require significant funding from industry, private or public institutions, would they be able to reverse the current unfavorable trend for CAS.
Conclusion
CAS has evolved dramatically over the last two decades, yet it continues to be the subject of heated discussion and scrutiny. Large studies conducted over the last decade have proven that CAS can give a safe and long-lasting option for revascularization of carotid stenosis when performed by trained operators. Some would argue that CAS is currently the standard of therapy for certain high-risk patients. While the achieved results of CAS are comparable to those of CEA, more improvements, particularly in the lowering of perioperative stroke rate, are likely to be required before the treatment can be considered equivalent to or standard of care for all patients. In the future, further data, including comparisons to best medical therapy, will be required, particularly in the asymptomatic individual. In view of the tremendous improvements in best medical therapy over the last few decades, this work should assist in completely defining the role of CAS.