Introduction
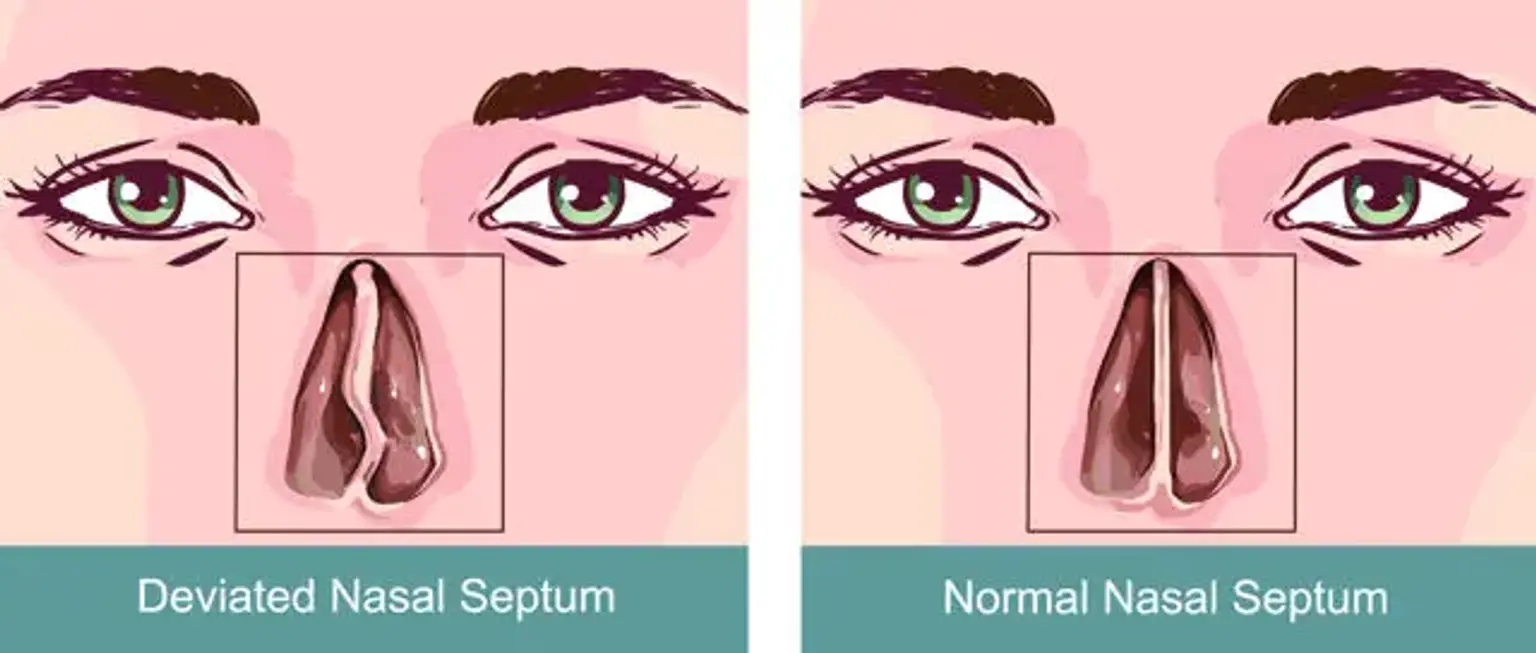
A deviated septum occurs when the thin wall (septum) inside the nose that divides the nostrils is off-center or crooked. This condition can cause significant breathing difficulties, frequent sinus infections, and persistent nasal congestion. For many, Septoplasty, a surgical procedure designed to correct a deviated septum, provides relief.
Septoplasty is one of the most commonly performed nasal surgeries worldwide, aimed at restoring normal airflow by straightening the septum. The procedure not only improves breathing but can also alleviate other symptoms like snoring, sinus issues, and chronic headaches. If you’re struggling with persistent nasal problems, Septoplasty might be the solution.
Understanding a Deviated Septum
A deviated septum happens when the nasal septum, the cartilage and bone separating the two sides of your nose, is displaced or crooked. This can result from genetic factors, trauma (such as a nose injury), or developmental issues. In many cases, a deviated septum is present from birth, though it may become more noticeable over time.
Common symptoms include:
Difficulty breathing through one or both nostrils
Chronic sinus congestion and frequent infections
Snoring or disturbed sleep
Headaches
A significant deviation can lead to nasal airway obstruction, making it harder to breathe properly, especially at night. In severe cases, it can cause sinusitis (sinus infections) and contribute to problems with sleep and quality of life.
The Need for Deviated Septum Surgery
While mild deviations may not require surgery, more severe cases of a deviated septum can cause significant discomfort and health issues. When symptoms like chronic sinus infections, breathing difficulties, or snoring persist despite medical treatments (e.g., nasal sprays, antihistamines), surgery may be recommended.
Septoplasty is performed when:
Non-surgical treatments don’t work
Breathing through the nose is consistently difficult
Chronic sinus infections or congestion are present
The patient is suffering from disturbed sleep or snoring
By straightening the septum, Septoplasty improves airflow and addresses the underlying causes of congestion and sinus issues, significantly enhancing the patient’s quality of life.
How Septoplasty Works: Step-by-Step Process
Consultation and Pre-Surgical Assessment: The first step is a thorough consultation with a qualified ENT (Ear, Nose, and Throat) specialist. They will perform a physical exam and may order imaging tests (like X-rays or CT scans) to evaluate the septum’s condition.
The Surgical Procedure: Septoplasty is usually performed under general anesthesia, though local anesthesia is sometimes an option. The surgeon makes an incision inside the nose to access the septum, where they will straighten or remove the deviated portions of cartilage or bone. The procedure typically takes 30 minutes to an hour.
Duration and Setting: Septoplasty is an outpatient procedure, meaning patients can go home the same day. However, if the surgery is more extensive or involves other procedures like rhinoplasty, a short hospital stay may be required.
Anesthesia Options: While general anesthesia is most commonly used, local anesthesia with sedation can also be an option for some patients, depending on the complexity of the procedure and the patient's health status.
Risks and Benefits of Deviated Septum Surgery
Like any surgery, Septoplasty carries some risks. However, these are generally low when performed by a skilled surgeon in a reputable setting.
Common Risks:
Infection: As with any surgery, there is a risk of infection at the incision site.
Bleeding: Mild bleeding is common, but more severe bleeding can occur in rare cases.
Scarring: Though incisions are typically inside the nose, scarring can still happen.
Changes in Sensation: Some patients experience temporary numbness or altered sensation in the nose or upper gums.
Benefits:
Improved Breathing: The most significant benefit is improved airflow, making it easier to breathe through the nose.
Reduced Sinus Infections: Surgery can help prevent recurrent sinus infections caused by chronic congestion.
Better Sleep: With improved airflow, patients may experience better quality sleep and reduced snoring.
Overall Quality of Life: The procedure can greatly enhance daily comfort, with fewer symptoms like nasal congestion or sinus pressure.
Post-Operative Complications and How to Avoid Them
Though complications after Septoplasty are rare, it's important to be aware of potential risks and how to minimize them.
Common Complications:
Infections: A minor risk that can be minimized with proper hygiene and follow-up care.
Persistent Bleeding: Some patients may experience ongoing bleeding, especially in the first few days after surgery.
Septal Perforation: Rarely, a small hole may form in the septum during the procedure, though it can often be repaired.
Prevention:
Proper Aftercare: Follow all post-surgical instructions carefully, including taking prescribed medications and attending follow-up visits.
Rest: Avoid any activities that could put strain on your nose, including exercise and heavy lifting.
Monitor for Infection: Watch for signs of infection (redness, warmth, or excessive pain) and contact your doctor immediately if you suspect any issues.
Recovery After Septoplasty Surgery
Recovery from Septoplasty typically takes about one to two weeks, though full healing may take several months. Post-surgery, you’ll need to rest and avoid strenuous activities that could strain your healing nose.
What to Expect:
Initial Days: You may experience mild pain, swelling, and nasal congestion. Over-the-counter pain relievers can help manage discomfort.
Nasal Packing: In some cases, the surgeon may insert soft packing into the nose to help control bleeding. This will be removed within a day or two.
Swelling and Bruising: Swelling around the nose and eyes is common and should subside within a week or two.
Follow-Up Appointments: Regular check-ups are crucial to ensure proper healing and to remove any packing or splints.
It’s essential to avoid blowing your nose or engaging in any activity that could strain the healing process.
Septoplasty vs. Rhinoplasty
While Septoplasty and Rhinoplasty are both nasal surgeries, they serve different purposes. Septoplasty is a functional procedure designed to correct a deviated septum and improve breathing, while Rhinoplasty is cosmetic surgery aimed at changing the shape or size of the nose.
Key Differences:
Purpose: Septoplasty focuses on improving nasal function, whereas rhinoplasty alters appearance.
Insurance Coverage: Insurance may cover Septoplasty if it’s medically necessary, but Rhinoplasty is often considered cosmetic and may not be covered by insurance.
Combining Procedures: In some cases, patients may choose to combine Septoplasty with Rhinoplasty to address both functional and aesthetic concerns at once. This combined approach can provide both a more attractive nose and improved airflow, though it requires careful planning and a skilled surgeon.
Safety Protocols in Deviated Septum Surgery
Ensuring safety during Septoplasty is critical. Choosing a qualified, experienced surgeon is the first step to a successful procedure. Look for a board-certified ENT specialist with experience in nasal surgeries.
Key Safety Considerations:
Accredited Facilities: Ensure the surgery is performed in a certified surgical center with modern equipment and monitoring systems.
Pre-Surgical Evaluation: Before surgery, patients undergo a thorough assessment to evaluate their medical history, allergies, and overall health to minimize risks.
Post-Operative Monitoring: After the procedure, proper care and follow-up are crucial to monitor for any complications.
By following established safety protocols, risks can be minimized, ensuring a smoother recovery and better outcomes.
The Cost of Deviated Septum Surgery
The cost of Septoplasty can vary depending on factors like location, surgeon’s experience, and the complexity of the surgery. On average, the procedure can cost anywhere from $3,000 to $10,000.
Factors Influencing Cost:
Surgeon’s Fees: Experienced surgeons may charge more for their expertise.
Hospital or Surgical Center Fees: The facility where the surgery is performed plays a role in the cost.
Insurance: Many insurance plans cover Septoplasty if the procedure is deemed medically necessary. Be sure to check with your insurance provider for details.
Additional Costs: Don’t forget to factor in post-operative care, such as follow-up visits, medications, and any potential complications.
If you don’t have insurance coverage, financing options may be available to help manage the costs.
Real-Life Case Studies: Success Stories
Many patients who undergo Septoplasty report significant improvements in their quality of life. For instance, Sarah, a 32-year-old patient who struggled with chronic sinusitis and sleepless nights due to her deviated septum, experienced relief within weeks after surgery. She now enjoys uninterrupted sleep and fewer sinus infections.
Another patient, Michael, had difficulty breathing through one side of his nose for years. After his Septoplasty, he reported much easier breathing and no longer experiences the pressure and pain that once accompanied sinus congestion.
These success stories show that Septoplasty can dramatically improve a patient’s daily life, making it a life-changing procedure for those struggling with severe nasal issues.
FAQs about Deviated Septum Surgery
1. How soon can I return to work after Septoplasty?
Most patients can return to work within 7-10 days, depending on the type of work they do. However, heavy physical activity should be avoided for at least 2-4 weeks.
2. Is Septoplasty painful?
The surgery itself is done under anesthesia, so there’s no pain during the procedure. Post-operative discomfort is generally mild and can be managed with pain medication.
3. How long does it take to see results?
You may start feeling better in just a few weeks, but complete healing can take 6 months to a year. The results, such as improved airflow, are often noticeable immediately after the surgery.
4. Can Septoplasty be combined with rhinoplasty?
Yes, Septoplasty and Rhinoplasty can be performed together if both functional and aesthetic concerns need to be addressed.
Long-Term Results and Effectiveness
The long-term results of Septoplasty are generally positive, with many patients enjoying improved nasal function for years to come. After the surgery, patients can expect:
Improved Breathing: The most noticeable result is better airflow, leading to easier breathing through the nose.
Fewer Sinus Infections: Chronic sinus problems often improve or completely resolve after the surgery.
Better Sleep Quality: With improved airflow, many patients report a decrease in snoring and improved sleep quality.
However, while most patients experience long-lasting benefits, some may require additional treatment if symptoms recur over time. It's important to follow your surgeon’s advice and attend follow-up appointments to ensure ongoing success.
Global Popularity of Deviated Septum Surgery
Septoplasty is a popular procedure worldwide, not only in the United States but also in Europe, Asia, and Latin America. As awareness of the benefits of nasal surgery increases, more people seek help for deviated septum symptoms.
In countries like the U.S. and the U.K., Septoplasty is commonly covered by insurance if it’s considered medically necessary. In some places, cosmetic concerns are also considered, with people opting for Septoplasty alongside rhinoplasty to improve both form and function.
The procedure is increasingly recognized for its ability to significantly improve the quality of life by addressing breathing problems, sleep apnea, and chronic sinus issues, making it highly sought after globally.
Choosing the Right Surgeon for Septoplasty
Selecting a highly skilled surgeon is crucial for a successful outcome. When choosing a surgeon for Septoplasty, consider the following:
Board Certification: Ensure your surgeon is board-certified in ENT (Ear, Nose, and Throat) surgery or facial plastic surgery.
Experience: Look for a surgeon with extensive experience in nasal surgeries, particularly Septoplasty.
Patient Reviews: Reading patient testimonials and reviews can give you insight into the surgeon’s approach and results.
Initial Consultation: A thorough consultation is essential to discuss your symptoms, surgical options, and expected outcomes. The surgeon should provide clear answers and explain the risks and benefits of the procedure.
A good surgeon will ensure you are well-informed and prepared for both the surgery and recovery process, increasing your chances of a positive result.
Preparing for Septoplasty Surgery
Preparation for Septoplasty is crucial to ensure a smooth and successful procedure. Your surgeon will provide detailed instructions, but here are some general guidelines to help you get ready for surgery:
1. Pre-Surgical Consultation:
During the consultation, your surgeon will evaluate your medical history, perform a physical exam, and may request imaging tests (e.g., X-rays or CT scans) to assess the extent of your septal deviation.
Discuss any allergies, medications, or previous surgeries with your doctor to ensure the safest approach.
2. Avoid Certain Medications:
You may need to stop taking blood-thinning medications (e.g., aspirin, ibuprofen) at least two weeks before surgery to reduce the risk of bleeding.
3. Arrange for Post-Surgery Care:
It's essential to have a friend or family member available to drive you home after the surgery, as anesthesia can leave you groggy. Plan for someone to help you with household tasks during the recovery period.
What to Expect on the Day of Surgery
The day of surgery, you'll likely be at the surgical facility for several hours. Here’s a quick overview of what you can expect:
1. Anesthesia:
Septoplasty is usually performed under general anesthesia, so you will be asleep during the procedure. In some cases, local anesthesia with sedation may be used.
2. The Surgery Itself:
The surgeon will make incisions inside the nose to access the septum, then straighten or remove the crooked parts. The procedure typically takes 30 to 60 minutes, depending on the complexity.
3. Recovery Room:
After surgery, you’ll be monitored in a recovery room until the anesthesia wears off. Most patients can go home the same day, though more complex cases may require a brief hospital stay.
Adjusting to Life After Septoplasty
The first few days after Septoplasty can be a bit uncomfortable, but recovery is generally quick. Here's how to manage during the recovery period:
1. Managing Discomfort:
Expect mild discomfort, swelling, and bruising, especially around the eyes. This usually peaks within the first 48 hours and improves within a week.
Your doctor may prescribe pain relievers or recommend over-the-counter medications for pain management.
2. Swelling and Congestion:
Nasal congestion may persist for a few weeks as the nose heals. Some swelling is normal, but should gradually subside within a few days.
3. Activity Restrictions:
Avoid strenuous activities, including exercise and heavy lifting, for about 2-4 weeks. This helps prevent complications and ensures proper healing.
4. Follow-Up Appointments:
Regular follow-ups with your surgeon are important for monitoring your progress and removing any nasal packing or splints.
Conclusion
Septoplasty is a highly effective procedure for those suffering from a deviated septum and related symptoms. By correcting the septum, the surgery provides long-lasting benefits, including better breathing, reduced sinus infections, and improved sleep.
Whether you're dealing with chronic nasal congestion, snoring, or frequent sinus problems, Septoplasty can be life-changing. The procedure is safe, and recovery is relatively straightforward with proper care.
Consult with a skilled ENT surgeon to determine if Septoplasty is the right solution for your nasal issues. With the right preparation and aftercare, you'll be able to breathe easier and enjoy a better quality of life in no time.