Introduction
Uterine fibroids are non-cancerous tumors that develop in the wall of the uterus, affecting up to 80% of women by the age of 50. While many fibroids are symptom-free, others can cause significant issues, including heavy bleeding, pelvic pain, and even infertility. Traditional fibroid treatments have included invasive surgeries, but today, hysteroscopic fibroid removal offers a minimally invasive solution. This procedure has gained popularity globally due to its efficiency, reduced recovery time, and the ability to preserve fertility.
In this article, we’ll explore what hysteroscopic fibroid removal involves, the types of fibroids it treats, and the benefits it offers to patients.
What Are Uterine Fibroids?
Uterine fibroids are benign growths made up of muscle and fibrous tissue that form in the uterus. These growths vary in size from tiny, undetectable nodules to large masses that can distort the shape of the uterus. Fibroids are categorized into three types:
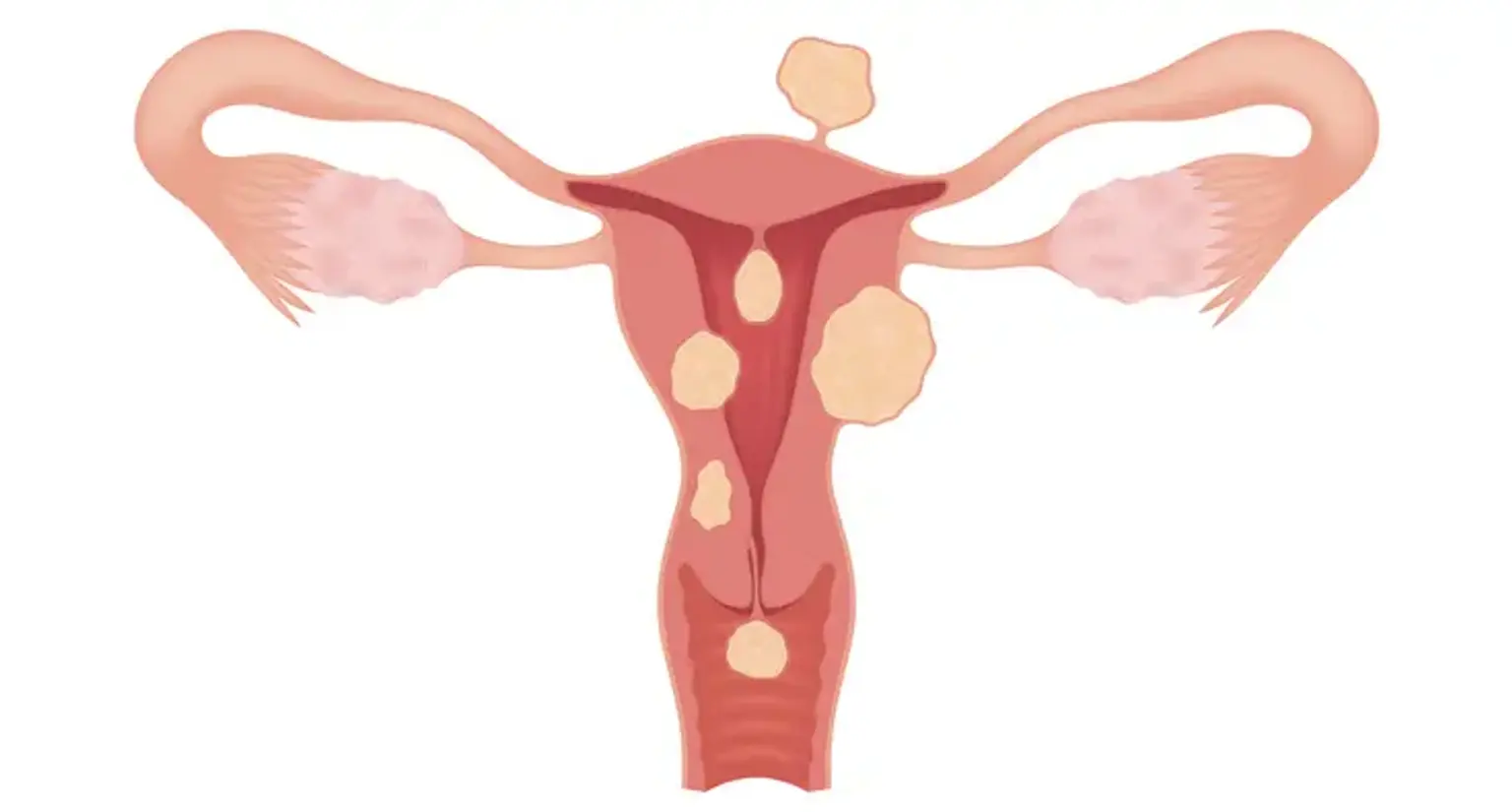
Submucosal fibroids: Located just under the lining of the uterus, these fibroids can significantly affect menstruation and fertility.
Intramural fibroids: The most common type, growing within the muscular wall of the uterus.
Subserosal fibroids: Found on the outer wall of the uterus, they often cause fewer symptoms.
While fibroids may not cause any symptoms, those that do can lead to problems like heavy menstrual bleeding, pelvic pain, and frequent urination. Submucosal fibroids, in particular, are most commonly associated with symptoms, and they often require surgical intervention for relief.
Understanding Hysteroscopy
Hysteroscopy is a medical procedure in which a thin, flexible tube with a camera (hysteroscope) is inserted through the cervix into the uterus to view the uterine cavity. It can be used both for diagnosis (detecting abnormalities) and treatment (such as fibroid removal). When fibroids are diagnosed, a hysteroscopic fibroid removal is an effective, minimally invasive solution.
During the procedure, the doctor inserts specialized surgical instruments through the hysteroscope to remove or shrink the fibroids. This technique is highly targeted and doesn't require large incisions, which means quicker recovery and fewer risks than traditional surgeries.
Types of Fibroids That Can Be Treated with Hysteroscopy
Not all uterine fibroids are suitable for hysteroscopic removal, as the procedure is best for submucosal fibroids. These fibroids are located just beneath the lining of the uterus, and they can interfere with menstrual cycles and fertility.
Submucosal fibroids are the primary candidates for hysteroscopic treatment because they grow into the uterine cavity and directly affect its lining. Removing them with a hysteroscope can significantly improve symptoms like heavy bleeding and pain.
Intramural fibroids (which grow within the muscular wall of the uterus) may also be treated using hysteroscopy if they have a significant submucosal component. However, larger or more deeply embedded intramural fibroids may require other surgical options.
Subserosal fibroids (located on the outer uterus) usually do not require hysteroscopy, as they are less likely to cause symptoms related to the uterine cavity, but they can be removed with other methods if necessary.
Hysteroscopic fibroid removal is effective for smaller fibroids that are in direct contact with the uterine lining, and it’s a great choice when the goal is to preserve fertility and avoid major surgery.
How Hysteroscopic Fibroid Removal Works
Hysteroscopic fibroid removal is a straightforward procedure that typically lasts between 30 minutes to an hour. Here’s how it works:
Anesthesia: The patient is given either local or general anesthesia depending on the complexity of the procedure.
Insertion of Hysteroscope: The hysteroscope is gently inserted through the cervix and into the uterus. The camera allows the surgeon to visualize the fibroids clearly.
Fibroid Removal: Using specialized instruments, the surgeon removes the fibroid or breaks it into smaller pieces. In some cases, the fibroid is vaporized using laser or other energy-based methods.
Post-Procedure Care: After the fibroid is removed, the surgeon may perform a final check to ensure that the uterus is free of any remaining fibroid tissue. The patient is then monitored for a short period before being discharged.
Because the procedure is minimally invasive, patients can often go home the same day and experience minimal discomfort. It is also effective for treating submucosal fibroids, which are difficult to treat through other methods.
Benefits of Hysteroscopic Fibroid Removal
There are several reasons why hysteroscopic fibroid removal is becoming a preferred choice for women with submucosal fibroids:
Minimally Invasive: Hysteroscopy requires no large abdominal incisions, reducing the risk of infection, scarring, and pain compared to traditional surgery.
Faster Recovery: Since there is minimal tissue disruption, patients typically experience shorter hospital stays and can return to their normal activities within a few days. In many cases, patients can go home the same day.
Fertility Preservation: One of the most significant advantages is that hysteroscopic fibroid removal does not require removal of the uterus, so women looking to preserve their fertility can benefit greatly from this option.
Less Pain and Blood Loss: Because the procedure is minimally invasive, there is less post-operative pain and less bleeding during and after surgery.
High Success Rate: The success rate for hysteroscopic fibroid removal is generally high, especially when treating smaller fibroids. Most patients experience relief from symptoms such as heavy bleeding and pain after the procedure.
Is Hysteroscopic Fibroid Removal Effective for Heavy Bleeding?
One of the most common reasons women seek fibroid removal is to treat heavy menstrual bleeding. Fibroids, particularly submucosal fibroids, can cause excessive bleeding during menstruation due to their location within the uterus.
Hysteroscopic fibroid removal is highly effective in reducing or eliminating heavy bleeding caused by these fibroids. By directly removing the fibroid from the uterine lining, the procedure restores normal uterine function, leading to a significant reduction in bleeding.
Studies have shown that many women experience immediate relief from heavy periods following hysteroscopic treatment, with some even reporting regular, lighter periods afterward. The procedure has been found to be particularly beneficial for women who do not wish to undergo a hysterectomy but want to address fibroid-related symptoms.
In addition to heavy bleeding, hysteroscopic fibroid removal can help alleviate other fibroid-related symptoms like pelvic pressure and pain, contributing to an improved quality of life.
Pre-Surgical Assessments and Preparation
Before undergoing hysteroscopic fibroid removal, patients will need a thorough evaluation to ensure they are good candidates for the procedure. This typically includes:
Physical Examination: A doctor will assess the patient’s overall health and review their medical history.
Ultrasound or MRI: These imaging tests help determine the size, number, and location of the fibroids, ensuring the procedure is appropriate.
Blood Tests: To check for any underlying issues that could affect the surgery, such as anemia due to heavy bleeding.
Discussion of Anesthesia: The anesthesia team will discuss the type of anesthesia used during the procedure.
Proper preparation is key to ensuring a smooth procedure and recovery.
Recovery and Aftercare
One of the major benefits of hysteroscopic fibroid removal is the quick recovery time. Most women can resume normal activities within a few days. However, there are a few guidelines to ensure a smooth recovery:
Rest: It’s important to rest for the first 24–48 hours following the procedure to allow the uterus to heal.
Avoid Heavy Lifting: Patients should avoid strenuous activities, such as lifting heavy objects, for at least 2 weeks.
Pain Management: Mild cramping or discomfort may occur. Over-the-counter pain relievers are usually sufficient, but stronger medication may be prescribed if needed.
Follow-Up Appointments: A follow-up visit is usually scheduled within 1–2 weeks to check for any complications and monitor healing.
While the recovery process is relatively quick, it’s important to follow the doctor’s guidelines for the best results.
Global Popularity and Accessibility
Hysteroscopic fibroid removal has become increasingly popular worldwide due to its efficiency and minimal downtime. This procedure is widely available in most developed countries, particularly in Europe and North America, where advanced medical facilities offer state-of-the-art technology.
Many women prefer this option because it provides a safe and effective way to treat fibroids without requiring more invasive procedures like hysterectomy. Additionally, the cost-effectiveness of hysteroscopic fibroid removal compared to traditional surgeries makes it an attractive choice for many patients.
Global accessibility has also been boosted by the growing awareness of the procedure. In countries with emerging healthcare systems, hysteroscopy is becoming more widely offered, with increasing numbers of practitioners trained to perform the procedure safely and effectively.
Safety Protocols and Risks of Hysteroscopic Fibroid Removal
Like any medical procedure, hysteroscopic fibroid removal comes with some risks, though it is generally considered safe. The procedure is minimally invasive, reducing many of the complications seen with traditional surgery. However, it’s important to be aware of potential risks:
Infection: Although rare, infections can occur following the procedure. Proper hygiene and care are crucial.
Uterine Perforation: In some cases, the instruments used may puncture the uterine wall, requiring further treatment.
Bleeding: Some bleeding is expected, but excessive bleeding may require intervention.
Anesthesia Risks: As with any procedure involving anesthesia, there are risks associated with reactions to anesthesia.
To minimize these risks, it’s vital to choose a qualified surgeon and follow pre-operative and post-operative instructions carefully.
Cost of Hysteroscopic Fibroid Removal
The cost of hysteroscopic fibroid removal can vary significantly based on factors such as location, the complexity of the procedure, and whether the patient has insurance coverage. On average, the cost can range from $5,000 to $15,000 in the United States, with the procedure being more affordable in countries with lower healthcare costs.
Insurance Coverage: Many insurance plans cover hysteroscopic fibroid removal if it is deemed medically necessary, especially if the fibroids cause symptoms like heavy bleeding or infertility. It’s important to check with your insurance provider to confirm coverage.
Out-of-Pocket Costs: For those without insurance, costs can vary depending on the hospital or clinic, location, and any additional treatments required during the procedure.
While the upfront cost can seem high, the minimally invasive nature of the surgery often leads to fewer post-operative expenses and a faster recovery, ultimately making it a cost-effective choice in the long run.
Impact on Fertility and Future Pregnancies
One of the most significant advantages of hysteroscopic fibroid removal is its ability to preserve fertility. Unlike a hysterectomy, which removes the uterus entirely, hysteroscopic fibroid removal focuses only on removing or shrinking the fibroids, leaving the uterus intact.
For women struggling with infertility due to submucosal fibroids, this procedure can increase the chances of a successful pregnancy. By removing the fibroids from the uterine lining, hysteroscopic fibroid removal helps improve the implantation environment, allowing for easier conception.
Studies show that women who undergo this procedure experience a significant increase in pregnancy rates, particularly those who had fertility issues caused by fibroids obstructing the uterine cavity.
However, it’s important to note that the success of the procedure also depends on the woman’s overall health, age, and the size and number of fibroids. A detailed discussion with the surgeon is essential to set realistic expectations.
Comparing Hysteroscopic Fibroid Removal to Other Fibroid Treatments
There are several options available for treating uterine fibroids, and the choice of treatment depends on factors like the size, location, and type of fibroids, as well as the patient’s symptoms and fertility goals. Here’s how hysteroscopic fibroid removal compares to other treatments:
Myomectomy (Open Surgery): Traditional myomectomy involves larger incisions and a longer recovery time. While it is effective for larger or deeply embedded fibroids, it comes with a higher risk of complications like infection and scarring.
Hysterectomy: This involves the complete removal of the uterus. While it is a permanent solution, it’s only recommended when the fibroids are causing severe symptoms and when preserving fertility is not a concern.
Uterine Artery Embolization (UAE): This non-surgical procedure involves cutting off the blood supply to the fibroids to shrink them. It’s effective for larger fibroids but is not suitable for submucosal fibroids, which are most often treated with hysteroscopy.
Medications: Hormonal treatments and other medications can help manage symptoms temporarily but do not offer a permanent solution. Medications are often used before or after surgical procedures.
Hysteroscopic fibroid removal stands out for its minimally invasive approach, shorter recovery time, and its ability to preserve fertility, making it an excellent choice for women with submucosal fibroids.
Common Concerns and Frequently Asked Questions
Many women have questions and concerns before undergoing hysteroscopic fibroid removal. Here are some of the most common FAQs:
Is the procedure painful?
Most women experience mild cramping or discomfort during the procedure, but general anesthesia is typically used, so patients are asleep and do not feel pain. Post-operative pain is usually mild and can be managed with over-the-counter pain relievers.
How long does the procedure take?
The surgery typically lasts between 30 minutes to 1 hour, depending on the number and size of the fibroids.
How soon can I return to work?
Recovery is generally quick, with many women returning to work in about 3 to 5 days, depending on the nature of their job.
Can the fibroids grow back?
While it is rare for fibroids to regrow after hysteroscopic removal, it is still possible. Regular follow-ups with your doctor can help monitor the uterine health.
Is hysteroscopic fibroid removal right for me?
This procedure is ideal for women with submucosal fibroids or those who want to preserve fertility. Women with larger, deeper fibroids may need alternative treatments like myomectomy or uterine artery embolization.
By addressing these concerns, patients can feel more confident in their decision to pursue this treatment.
Hysteroscopic Fibroid Removal and Emotional Well-being
Undergoing a medical procedure like hysteroscopic fibroid removal can have emotional effects, especially for women who have been suffering from symptoms such as heavy bleeding, pain, or fertility issues. The emotional relief after successful surgery can be just as important as the physical benefits.
Improved Quality of Life: Many women report feeling a sense of freedom after their fibroids are removed, especially those who have dealt with chronic pain or menstrual issues for years.
Restoring Fertility: For those struggling with fertility issues due to fibroids, the procedure offers hope for future pregnancies. Conception and pregnancy can significantly improve a woman’s mental and emotional well-being, boosting her confidence and satisfaction with life.
Addressing Anxiety and Stress: Though the procedure is minimally invasive, it is still important for patients to manage any anxiety or stress before surgery. Counseling or support groups can help women prepare emotionally and cope with any concerns about their health and the potential outcomes.
The emotional recovery post-surgery is just as important as the physical recovery. Support from family, friends, or even a therapist can help women navigate this journey.
Choosing the Right Surgeon for Hysteroscopic Fibroid Removal
When considering hysteroscopic fibroid removal, selecting a skilled and experienced surgeon is one of the most important decisions to make. Here’s what to look for:
Board Certification: Ensure that your surgeon is board-certified in obstetrics and gynecology, preferably with expertise in minimally invasive surgery.
Experience: Choose a surgeon who has performed multiple hysteroscopic fibroid removals and has a proven track record of success. Ask about their experience with different types of fibroids and their approach to surgery.
Patient Reviews and Testimonials: Reading reviews from other patients can help you gauge the surgeon’s approach, bedside manner, and the quality of care they provide.
Consultation: During the consultation, feel free to ask questions about the procedure, potential risks, recovery, and how they approach patient care. A good surgeon should be able to provide clear, comprehensive answers and make you feel at ease.
Long-Term Results and Effectiveness
Hysteroscopic fibroid removal offers long-term relief for many women by effectively removing the fibroids that cause symptoms like heavy bleeding, pelvic pain, and pressure. After the procedure, many women report an improvement in menstrual cycles, pain relief, and overall quality of life.
Symptom Relief: Most women experience a significant reduction in heavy bleeding and pelvic pain within the first few months after surgery. The results are often long-lasting, especially for women with smaller fibroids.
Recurrence of Fibroids: While fibroid recurrence is possible, it is relatively uncommon after hysteroscopic removal. However, if new fibroids develop, additional treatment may be needed.
The procedure is highly effective for those with submucosal fibroids, and long-term follow-up care is generally minimal, making it an attractive option for women seeking relief from fibroid-related symptoms.
Conclusion
Hysteroscopic fibroid removal offers a highly effective, minimally invasive solution for women suffering from symptoms caused by fibroids. The procedure provides significant relief from heavy bleeding, pelvic pain, and fertility issues, allowing women to regain control of their health and well-being. With quick recovery, minimal scarring, and the ability to preserve fertility, it’s an attractive alternative to more invasive treatments like hysterectomy.
While the procedure has its risks, proper planning, choosing a skilled surgeon, and following post-operative care instructions can help ensure the best outcomes. Advances in technology continue to improve the procedure, offering even better precision and patient satisfaction.
For many women, hysteroscopic fibroid removal is a life-changing solution, restoring not just their physical health, but also their emotional and reproductive potential. It’s a powerful option for those seeking a safe, effective, and less invasive way to address fibroids.