Gastric Bypass Surgery
Obesity is becoming more prevalent, with the United States presently ranked second in the world. Obesity (according to BMI) affected 40 percent of people in the United States, according to CDC data, involving around 100 million adults. Nearly 5 percent of the people were morbidly obese (BMI greater than or equal to 40). Obesity increases the risk of developing diabetes, malignancies, hypertension, hypercholesterolemia, obstructive sleep apnea, cardiovascular disease, cerebrovascular disease, acid reflux disease (GERD), osteoarthritis, and hepatic steatosis, among other comorbidities.
In 2008, the estimated yearly healthcare expenses of obesity in the United States were $200 billion, with the expense for just an obese person reaching $1,500 greater than those of a healthy weight, posing a major financial burden. The expense of addressing obesity-related disease in the U.k. is estimated to be 6 billion euro each year, rising to 11 billion euros by 2050, according to the National Health System.
The body mass index is a measurement of a person's relative weight in relation to their height, and it has a strong relationship with total body fat.
The definition of obesity as per WHO is having a BMI of 30 or more.
Obesity can be treated with nonoperative treatment or bariatric surgery. Dietary improvements, exercise, behavioral alterations, and prescription medication are all part of the nonoperative treatment plan. For the most part, diet and physical activity recommendations have been shown to be ineffective. A cross-sectional study employing Behavioral Risk Factor Surveillance on 11 thousand persons in the United States indicated that despite the majority of the population are trying to lose weight, only 20 percent successfully lower their energy consumption and exercise for 150 min on weekly basis. Pharmacological intervention has had poor long-term outcomes in weight management, with a mean weight decrease of just 4 percent observed.
What is Gastric Bypass Surgery
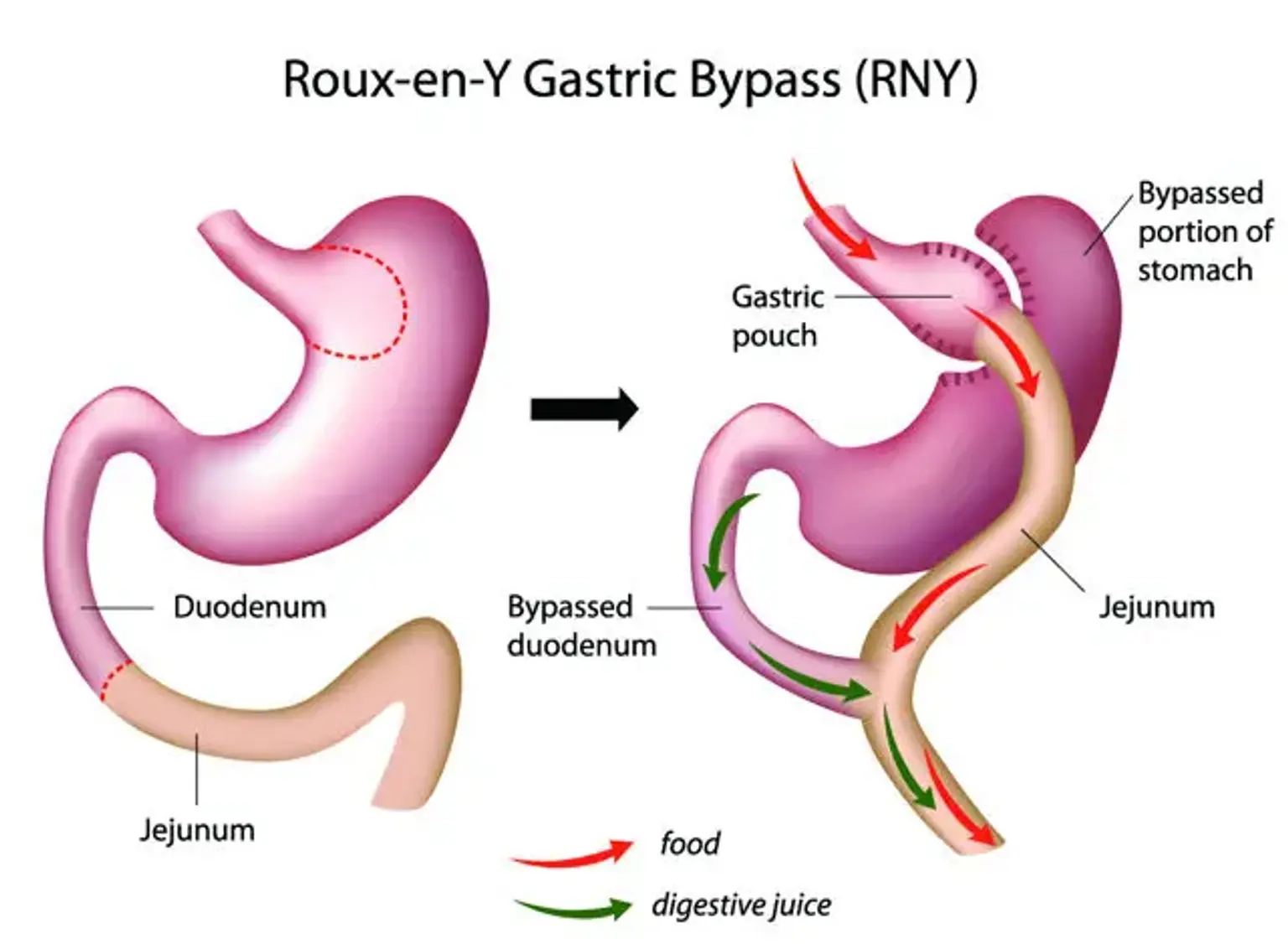
Gastric bypass surgery, also known as Roux-En-Y Surgery, is a laparoscopic technique involving the establishment of a stomach pouch and is undertaken to achieve dramatic and lengthy weight loss in highly obese individuals. The one-anastomosis gastric bypass is a less invasive alternative to the traditional Roux-en-Y bypass surgery.
Anatomy
The four anatomical regions of the stomach are explained below:
- The cardia is the superior part of the stomach located directly below the gastroesophageal junction.
- The fundus is a dome part of the stomach that is located near and lateral to the cardia.
- The body is located Just below the cardia and fundus; this is the main portion of the stomach.
- The pylorus is the angled notch between both the body and the pylorus is where it all begins. This structure corresponds to the L1 spinal level and is made up of the antrum, canal, and sphincter. It's a canal that runs from the stomach to the small intestine.
Curvatures of the stomach:
- Greater curvature– begins at the cardiac apex and travels in a long arc to create the fundus, body, and pyloric antrum's lateral borders. The gastroepiploic and short gastric arteries provide blood supply.
- Lesser curvature– begins at the gastroesophageal junction and extends to the angled depression on the stomach's medial surface. The left gastric artery and the right gastric artery supply the lesser curvature.
Anatomical surrounding structures:
- The stomach is connected to the esophagus and the left half of the diaphragm superiorly.
- The abdominal wall, diaphragm, left lobe of the liver, and larger omentum are all located anterior to the stomach.
- The smaller sac is located posterior to the stomach. The pancreas, left kidney, and suprarenal gland are retroperitoneal organs, while the spleen and splenic artery are intraperitoneal structures.
Connections to the peritoneum:
- The greater omentum is the double layer of peritoneum that runs through the peritoneal cavity and originates from the stomach's greater curvature. The greater omentum wraps around the transverse colon and joins to it. The greater omentum's purpose is to stick to inflamed tissues and prevent the disease from spreading throughout the peritoneal cavity.
- The lesser omentum is responsible for connecting the stomach to the liver. It originates in the stomach's minor curvature and proceeds to the liver.
The two omenta separate the peritoneal cavity into bigger and lesser sacs, which connect through the Winslow foramen.
Blood supply:
The celiac trunk and its branches provide a dense anastomotic system that supplies the stomach with blood.
- Right gastric artery – it is a branch of the common hepatic artery
- Left gastric artery: it is the third branch of the celiac trunk
- Right gastroepiploic artery: it is a branch of gastroduodenal artery (which is a branch of the common hepatic artery)
- Left gastroepiploic artery: it is a branch of the splenic artery.
Drainage of the Venous System:
The short gastric veins and gastroepiploic veins empty into the superior mesenteric vein, while the right and left gastric veins empty straight into the hepatic portal vein.
Innervation:
- The parasympathetic nerve supply to the stomach is provided by the vagus nerve (tenth cranial nerve).
- The thoracic spinal cord sections 6,7,8,9 give rise to the greater splanchnic nerve, which offers sympathetic nerve supply to the stomach.
Gastric Bypass Surgery Requirements
In today's world, there are certain indications for gastric bypass surgery. A physician may perform this operation in rare cases of gastric outlet obstruction caused by malignancies or peptic ulcers.
The National Institutes of Health released a consensual statement regarding bariatric surgery patient selection. Patients who met one of the following criteria were deemed eligible for surgery:
- BMI of more than 40
- BMI of 35-40 with one of the following obesity-related conditions:
- type 2 diabetes
- Pickwickian syndrome
- obesity-associated cardiomyopathy
- disabling sleep apnea
- osteoarthritis disrupting daily activity
Patients must have tried and failed to reduce an appropriate amount of weight with guided diet adjustments to be considered for gastric bypass surgery. Individuals must also adhere to postoperative dietary and exercise guidelines.
Contraindications of Gastric bypass Surgery
Absolute contraindications
- Pregnancy
- End-stage renal disease
- Unstable coronary artery disease
- Severe heart failure
- Cirrhosis
- Portal hypertension
Relative Contraindications
- Crohn’s disease
- Psychosocial issues, such as drug or alcohol abuse.
- Patients with severe intellectual disabilities are unlikely to be suitable candidates because a high level of patient awareness of the risk and lifestyle implications of surgery must be demonstrated.
- Patients with epilepsy should have their drugs reviewed because bypass surgery affect absorption, as result, cautious decision-making should be sought.
Equipment of Gastric Bypass Surgery
Although there are numerous procedures for performing a gastric bypass surgery, many of the steps and equipment needed are similar and include the following:
- Orogastric tube
- Nathanson liver retractor
- Lange Bach retractors
- Artery clips
- A 30-degree laparoscope
- A light source and monitor
- Gas insufflator
- Hasson trocars
- Three bowel-safe graspers
- Laparoscopic ultrasonic dissector (E.g.: harmonic scalpel)
- Electrocautery equipment
- Laparoscopic suction irrigator
- Laparoscopic clips
- Medium wound protector
- Laparoscopic linear cutting stapler
- Scalpel
Personnel
Before being considered for bariatric surgery, patients must be evaluated by a multidisciplinary team. A nutritionist, a mental specialist, the surgical team, and the primary care physician are among those involved. The following members are required for the operative component:
- Anesthesiologist
- Chief surgeon
- Assistant scrub nurse
- Circulatory nurse
Preparation
All patients should have an endoscopy with H. pylori screening, abdomen ultrasound, pulmonary function tests(spirometry), and a routine laboratory assessment performed prior to surgery.
Patients' risk classification is a field of study that aims to improve which client groups are offered gastric bypass surgery.
The obesity Surgery-Mortality Risk Score (OS-MRS), which has been approved to be used in gastric bypass surgery, consists of the subsequent items:
- The male gender
- The age greater or equal to 45
- BMI greater or equal to 50
- The presence of high blood pressure
- Recognized risk of thromboembolic conditions.
Low-risk patients (class A): 0-1 points.
Moderate-risk patients (class A): 2-3 points.
High-risk patients (class A): 4-5 points.
Class C patients are the most frequently involved in gastric bypass surgery.
Preoperative antibiotics and venous thromboembolism prevention measures are administered to the patients half an hour before the surgery. In the preoperative zone, cutters are used to cut belly hair. A foley catheter is inserted after anesthesia is administered, and an orogastric line is placed in the stomach.
Gastric Bypass Surgery Technique
The following are some of the most prevalent approaches and variants used by surgeons in gastric bypass surgery:
- Setup and entry into the abdominal cavity
- Creation of the Roux-limb
- Jejuno-jejunal anastomosis
- Creation of the gastric pouch
- Gastro-jejunal anastomosis
- Endoscopy
- Closure
The patient is in a flat spread-legged position while being under general anesthesia. Once the patient is prepped and draped, the chief operator stands in between legs, and the monitor is placed above the patient's head. It can be difficult to establish pneumoperitoneum in extremely obese individuals. The Veress needle is most usually put in the right hypochondrium, with an optical trocar inserted 3-5 cm above the umbilicus. Additional 12 mm ports are inserted in the left and right upper quadrants, respectively. To withdraw the liver, a 5 mm port and Nathanson retractor are put into Martin's arm.
Creation of Gastric Pouch
Putting the patient in reversed Trendelenburg, pulling the left lobe of the liver away with a Nathanson retractor, and pulling the omentum inferiorly allows for proper access to the gastroesophageal junction.
The diaphragm's left crus and gastro-hepatic ligament are exposed by starting cutting at the angle of His. To mobilize the stomach, the pars flaccida and retro-gastric attachments are separated. The lesser sac is entered through the lesser curvature of the left gastric artery and vein, which separates neurovascular branches from the artery and vein.
The ideal gastric pouch is up to 30 cc in capacity and mostly comprises the stomach's lesser curvature. With long-term follow-up, this approach has shown consistent weight loss for the past 15 years. Starting at the lower boundary of the oblique fat pad, straight staplers are pushed transversely. A bite of 2–3 cm is taken. Then, the straight stapler is discharged vertically towards His angle.
Creation of Biliopancreatic Limb
The biliopancreatic limb (the afferent limb) is made up of the duodenum and proximal jejunum, which are connected proximally to the remaining stomach. Digestive enzymes from the stomach, hepatobiliary system, and pancreas are found in the limb. In a conventional gastric bypass, the biliopancreatic limb is created by measuring nearly 40 cm from the Treitz ligament and dividing it with a stapler.
Creation of Jejunojenuostomy
The roux limb is measured from the jejunal division point 75 to 150 cm, with an average of 120 cm. At this point, the biliopancreatic limb is anastomosed to the distal segment of the jejunum, forming a side-to-side jejunojejunostomy referred to as the JJ anastomosis.
Creation of Gastrojejunostomy
- Retro-colic retro-gastric: creating a defect in the transverse mesocolon and moving the Roux limb posterior to the remaining stomach. This produces a third possible place for an internal hernia to form, which must be sealed before the treatment is completed.
- Ante-colic ante-gastric: the Roux limb is brought anterior to the transverse colon and prior to the residual stomach in this position. In all procedures, the gap between both the roux limb mesentery and the transverse mesocolon must be sealed with suture, in addition to the space generated by the jejunojejunal anastomosis mesenteries.
Test for Leak
An upper endoscopy leak test is conducted before the procedure is completed when the gastrojejunostomy is apparent. The gastric pouch and gastrojejunostomy are immersed in saline while the patient is in Trendelenburg. To test patency, an endoscope is pushed through the gastrojejunostomy and subsequently expanded with gas. The submerged anastomosis is examined for bubbles, which could suggest a leak. When checking for a leak, some surgeons prefer to use methylene blue dye rather than gas.
Post Operative Care
In terms of post-procedure care and length of stay, protocols differ. an overnight stay is safe for the majority of patients. As same discharge has been linked to higher mortality and morbidity rates.
Side Effects of Gastric Bypass Surgery
Early Complications
- Anastomotic leak: it is a potentially deadly condition. It usually shows up within a day and can happen in as many as 3 percent of the total instances. A leak test conducted during surgery can help to reduce the risk of leakage. T tube implantation or the same laparoscopy and correction may be required. Due to their comorbidities and the catabolic condition that is unavoidable with this operation, these patients' healing is often delayed.
- Hemorrhage: the patient can bleed from anastomoses and staple lines and is more likely to resolve spontaneously, but it may necessitate transfusions while waiting for it to stop.
- Early bowel obstruction: it can develop due to the Roux-en-O mistake, in which the closed-loop blockage is caused by misidentification of Roux and BP limbs. Iatrogenic stricture at the JJ anastomosis, port site hernia, and small bowel volvulus can all cause early intestinal blockage.
- Venous thromboembolic disease: it is the most prevalent cause of death after gastric bypass surgery. The thrombo-embolic disorder is responsible for 50% of all deaths following gastric bypass surgery. Periodic calf pumps, compressive stockings, and pharmacologic prophylaxis for at minimum a week after surgery are all important preventative measures.
- Marginal ulcers: the development of a peptic ulcer on the jejunal mucosa at the gastrojejunal anastomosis. It is found in 1 to 16 percent of patients who undergo gastric bypass surgery. Acid injury to the largely exposed jejunal mucosa causes the disease.
- Gastrogastric fistula: it is an aberrant connection between the artificially formed pouch and the remaining stomach portion. It affects about 1 to 2 percent of individuals who have a divided stomach during gastric bypass surgery. A GGF can be caused by an inadequate stomach transection, anastomotic leakage, marginal ulcer perforation, or foreign body erosion.
Late Complications
- Internal herniation: it might happen in one of three ways during gastric bypass surgery. Hernia can arise after bowel herniation due to a defect produced between the alimentary limb's jejunal mesentery and the transverse mesocolon. The other two hernias can occur at the JJ anastomosis mesenteric defect or at the mesocolic defect if the Roux limb crosses retro-colic. The intestinal structure changes as weight is reduced, and mesenteric abnormalities can be emphasized or generated. Subacute symptoms such as post-prandial pain or bloating are common, although acute symptoms such as strangulation can also occur.
- Gastrojejunal anastomosis stricture: Excess tension and key technologies of the join-making procedures are contributing issues.
- Micronutrient deficiency: it can develop and lifelong supplemental therapy is necessary to avoid these deficits caused by intestinal absorption loss in the DJ region. Thiamine, vitamin B12, folic acid, iron, zinc, and vitamin D are all common deficits.
- Gallstone development: it can occur in up to 30 percent of people who lose weight quickly. Endoscopic retrograde cholangiopancreatography is unable to treat common bile duct stones in patients having bypass surgery. As a result, during laparoscopic cholecystectomy, on-table cholangiography is often used to rule out this possibility.
- Dumping syndrome: due to rapid transit of meals into the anastomosed jejunum at the GJ anastomosis, which manifests as a post-prandial malaise.
- Inability to reduce weight: It may occur despite a surgically well-performed treatment. Weight loss following bypass might be difficult to maintain for some people, owing to patients' resumed binge-eating patterns.
Gastric bypass has a death rate of about 2 per 1000, which is greater than both sleeve gastrectomy and gastric banding, which have the lowest mortality of the three.
How Long Does Gastric Bypass Surgery Take
In the operating room, the camera lens is attached to a monitor screen. This allows the operator to see within the stomach while doing the procedure, which takes around two to three hours.
Long Term Diet After Gastric Bypass Surgery
We advise our patients to bring a 24-hour dietary recall to their visit to assess proper nutrition. We advise them to drink at least 3L of water every day and stay away from sugary drinks and alcohol. Because of the limited size of the stomach pouch, which causes the individual to take fewer amounts of food, the diet following gastric surgery may be insufficient. Consumption of protein is frequently a concern, with most people consuming less than of optimum for body weight. Most patients can ingest 0.8–1 g of protein/kg of ideal body weight from a combination of foods and liquid supplements, resulting in a daily protein intake of 60–80 g.
The following are five guidelines for fluid consumption (in order to encourage fluid intake and improve satiety between meals):
- No liquids during meals; begin liquids at least 30 minutes after a meal. It's critical not to overload and expand the stomach pouch.
- Sip drinks rather than using a straw, which increases the amount of air swallowed.
- A daily hydration intake of at least 1.5 liters (6 cups) is recommended. High-protein liquid supplements, skim milk, and sugar-free noncarbonated beverages should all be included. It is preferable to drink decaffeinated coffee or tea.
- When you feel full, stop eating and drinking. When the stomach pouch is overfilled, it stretches, resulting in greater intake.
- Carbonated beverages should be avoided since the gas bubbles may strain the pouch.
Gastric Bypass Surgery Cost
The surgical admission for a Roux-en-Y gastric bypass (RYGB) costs between $20 000 and $30 000 (including the procedure and immediate preoperative, intraoperative, and postoperative treatments).
Conclusion
The Roux-en-Y gastric bypass is a malabsorptive surgery used to help people who have a BMI of 40 or more to lose weight, or who have a BMI of 35 or more and have obesity-related problems. Gastric bypass surgery can be done openly, laparoscopically, or robotically. The laparoscopic gastric bypass is the second most popular weight-loss operation. It has clear economic and patient satisfaction advantages over the standard open technique, with similar results. After laparoscopic gastric bypass, patients should plan to lose about 60 percent of their extra weight and have excellent long-term management of obesity-related complications. A laparoscopic gastric bypass can be done with low morbidity and great results once a doctor has gained knowledge. Following up after gastric bypass is crucial and necessitates a multidisciplinary approach. For the vast majority of patients, the advantages much outweigh the dangers, and they are likely to enjoy better and longer lives as a result of surgery. Patients must understand that the surgery is merely a tool and that reducing weight and maintaining it off will necessitate considerable effort on their side, especially in terms of healthy eating and exercise. Follow-up is crucial for achieving the finest long-term outcomes.