Introduction
Gynecological endoscopic procedures have revolutionized how women’s health conditions are diagnosed and treated. These minimally invasive techniques, including laparoscopy and hysteroscopy, provide a way to manage conditions like fibroids, ovarian cysts, endometriosis, and more, with less risk and shorter recovery times compared to traditional surgeries.
With their global popularity, these procedures are now widely available across the world. The use of small incisions, specialized instruments, and cameras allows gynecologists to perform detailed surgeries with precision, reducing the need for large cuts and lengthy recovery times. Minimally invasive gynecology has thus become the go-to choice for many patients and practitioners.
What Is Laparoscopy?
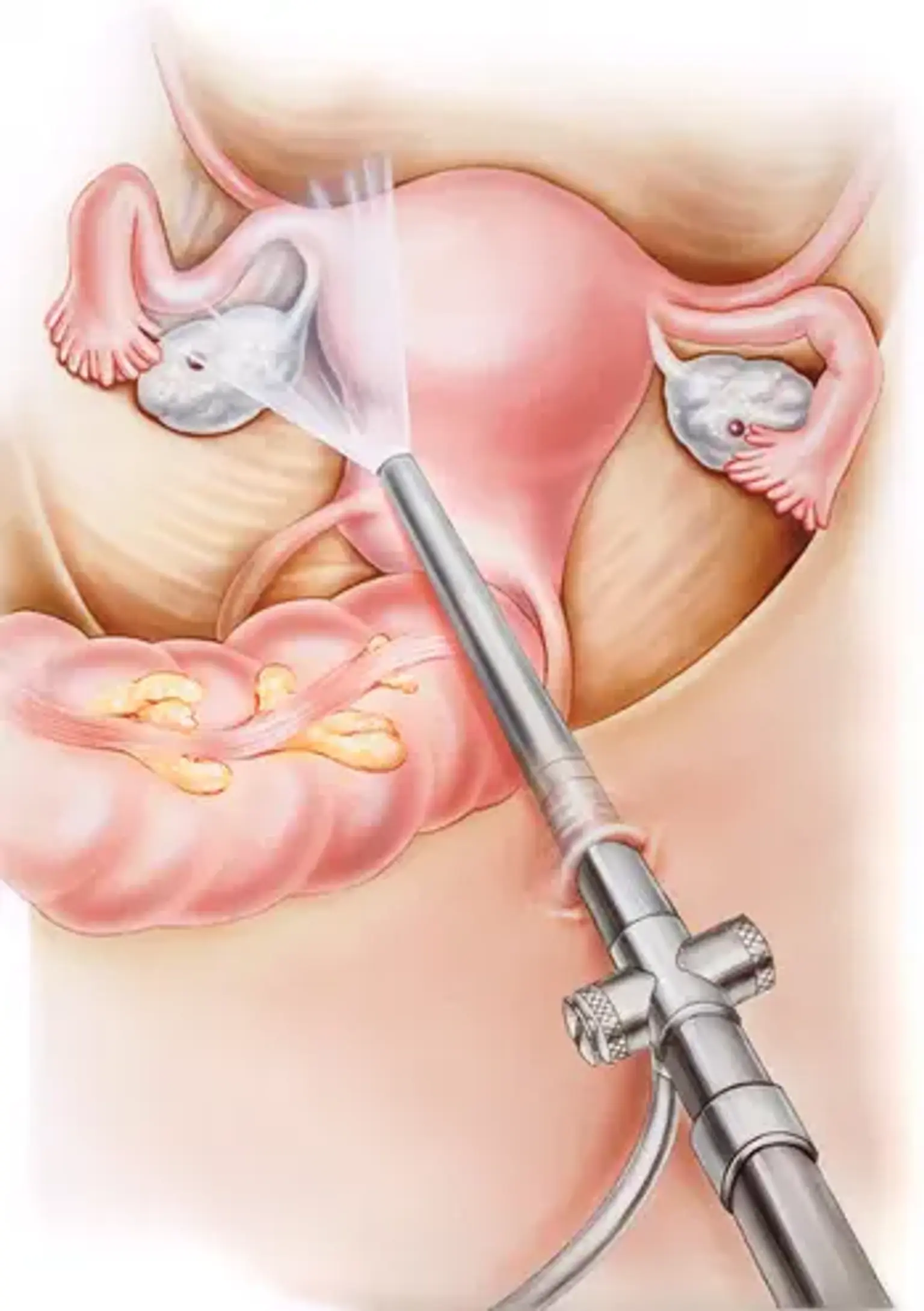
Laparoscopy is a surgical procedure used to view and treat conditions in the pelvic and abdominal areas, such as ovarian cysts, fibroids, and endometriosis. During the procedure, a small camera (laparoscope) is inserted through tiny incisions in the abdomen. The surgeon uses it to see and treat the condition with specialized tools.
One of the biggest advantages of laparoscopy is its minimally invasive nature. Patients experience shorter recovery times, less pain, and smaller scars compared to traditional open surgeries. For conditions like endometriosis or PCOS, laparoscopy allows doctors to remove cysts, endometrial tissue, or other growths with precision, improving fertility outcomes.
What Is Hysteroscopy?
Hysteroscopy is another important gynecological procedure that involves inserting a thin tube with a light and camera (hysteroscope) into the uterus through the cervix. It’s primarily used to diagnose and treat uterine conditions like fibroids, polyps, adhesions, and abnormal bleeding.
This procedure is essential for fertility preservation. It allows doctors to remove growths or clear blockages, improving the chances of pregnancy. In many cases, hysteroscopy is used as a diagnostic tool to investigate abnormal uterine bleeding or to check the condition of the uterine lining, especially for women experiencing infertility.
Endometriosis and Its Treatment via Laparoscopy
Endometriosis is a common yet painful condition where tissue similar to the uterine lining grows outside the uterus, causing severe pelvic pain, heavy periods, and infertility. Laparoscopy is the gold standard for diagnosing and treating endometriosis. During the procedure, the surgeon can remove or destroy the endometrial tissue to relieve pain and improve fertility.
Laparoscopy is highly effective in treating endometriosis because it provides direct access to the affected areas, allowing for precise removal of tissue. Many women report significant improvements in pain and fertility following this treatment. Its minimally invasive nature means patients experience less discomfort, a quicker recovery, and fewer complications compared to traditional surgeries.
Common Conditions Treated with Gynecological Endoscopy
Gynecological endoscopic procedures like laparoscopy and hysteroscopy are highly effective in treating various gynecological conditions.
Ovarian Cysts: Using laparoscopy, ovarian cysts can be removed with minimal invasiveness. This technique ensures reduced scarring and faster recovery, making it ideal for women dealing with recurrent cysts or fertility issues.
Fibroids: Uterine fibroids are non-cancerous growths in the uterus that can cause heavy bleeding and pain. Laparoscopic myomectomy, which removes the fibroids, is a common procedure that preserves the uterus, benefiting women who wish to maintain fertility.
Abnormal Uterine Bleeding: Hysteroscopy is often used to diagnose the cause of abnormal uterine bleeding, whether it’s due to fibroids, polyps, or other uterine conditions. This procedure offers a way to both diagnose and treat these issues in a single session.
These procedures, whether through laparoscopy or hysteroscopy, are favored due to their ability to treat these conditions with precision and minimal disruption to the body.
Tubal Sterilization and Endoscopic Methods
Tubal sterilization is a permanent method of birth control where the fallopian tubes are blocked or cut to prevent pregnancy. Laparoscopic tubal sterilization is a popular option as it requires only small incisions and leads to a faster recovery.
Laparoscopic Sterilization: The procedure involves inserting a laparoscope to block or remove a part of the fallopian tubes. It’s a highly effective and minimally invasive option for women who are certain they no longer want children. The benefits of this approach include shorter hospital stays and quicker recovery times compared to traditional sterilization methods.
Advantages Over Traditional Surgery: Unlike traditional sterilization, which involves larger incisions and a longer recovery period, laparoscopic sterilization ensures less pain and quicker return to daily activities, making it a preferred choice for many women.
Cost of Gynecological Endoscopic Procedures
The cost of gynecological endoscopic procedures can vary significantly depending on the country, the complexity of the surgery, and whether the procedure is done in a private or public healthcare setting.
Cost Variability Around the World: In countries with advanced healthcare systems, such as the U.S. or the UK, the cost of procedures like laparoscopy and hysteroscopy can range from $3,000 to $10,000 or more. However, in countries with less expensive healthcare, the costs may be considerably lower, making these procedures more accessible to a broader population.
Insurance Coverage: Many insurance plans cover these procedures, especially when they are medically necessary for conditions like endometriosis, fibroids, or abnormal uterine bleeding. However, elective surgeries like tubal sterilization or cosmetic procedures may not be covered, leaving patients with significant out-of-pocket costs.
Out-of-Pocket Expenses: For patients without insurance or those seeking elective treatments, the cost can be a barrier. It’s important for patients to check with their healthcare provider about payment plans, financing options, or discounts that may be available to ease the financial burden.
Fertility and Gynecological Endoscopic Procedures
Gynecological endoscopy plays a pivotal role in addressing fertility issues. Both laparoscopy and hysteroscopy are used to treat conditions that affect a woman’s ability to conceive.
Fertility Preservation: For women with PCOS, endometriosis, or uterine fibroids, laparoscopy can help remove cysts, endometrial growths, or fibroids that interfere with fertility. This increases the chances of successful pregnancy by removing obstructions or damage to the reproductive organs.
Hysteroscopic Myomectomy for Fertility: Fibroids can obstruct the uterine cavity, making pregnancy difficult. Hysteroscopic myomectomy can remove these fibroids with minimal disruption to the uterus, significantly enhancing the likelihood of conception.
Ectopic Pregnancy Surgery: Laparoscopy is also used to treat ectopic pregnancies, where the fertilized egg implants outside the uterus. Laparoscopic surgery allows for the removal of the ectopic tissue while preserving the fallopian tube and minimizing future fertility risks.
These minimally invasive procedures offer hope to women facing infertility due to gynecological conditions.
Comparison of Laparoscopy vs. Hysteroscopy
Both laparoscopy and hysteroscopy are minimally invasive procedures, but they serve different purposes and are used for different types of gynecological issues.
Key Differences: Laparoscopy is performed by inserting a small camera through an incision in the abdomen, allowing the surgeon to see and treat issues in the pelvic and abdominal areas. It’s primarily used for diagnosing and treating ovarian cysts, endometriosis, fibroids, and tubal issues. On the other hand, hysteroscopy involves inserting a camera through the cervix into the uterus to diagnose and treat conditions like fibroids, polyps, adhesions, and abnormal bleeding.
When to Use One Over the Other: The decision between laparoscopy and hysteroscopy depends on the type of condition being treated. If the issue is within the uterus, hysteroscopy is preferred. For conditions involving the ovaries, fallopian tubes, or other abdominal structures, laparoscopy is the better choice. In some cases, both procedures may be performed together, offering a comprehensive approach to treatment.
Complementary Roles: While they are distinct procedures, laparoscopy and hysteroscopy are often complementary. For instance, a patient with endometriosis may need a laparoscopic surgery to remove tissue, and a hysteroscopy to clear the uterus of any adhesions or fibroids. Both can be done in a single surgical session, improving outcomes.
Safety Protocols and Qualified Practitioners
The safety of gynecological endoscopic procedures is paramount, and strict protocols are followed to minimize the risk of complications.
Who Can Perform These Procedures?: These procedures should be performed by highly skilled gynecologists or surgeons who are trained in minimally invasive surgery. Surgeons must have experience in laparoscopy or hysteroscopy, as these techniques require precision and expertise. Some medical centers also offer robotic-assisted surgery for even greater accuracy.
Pre-Surgical Assessments: Before undergoing any endoscopic procedure, patients will undergo a pre-surgical assessment. This includes medical history reviews, physical exams, and diagnostic tests (such as ultrasound or MRI) to determine the specific issue. These tests help ensure that the chosen procedure is appropriate and that the patient is in good health for surgery.
Safety Standards: Reputable medical institutions follow strict safety standards to minimize risks such as infection, blood loss, or injury to nearby organs. These standards are based on global guidelines and are constantly updated to reflect the latest advancements in medical technology. After the procedure, patients are closely monitored for any signs of complications.
Global Appeal of Gynecological Endoscopic Procedures
Gynecological endoscopic procedures have gained tremendous popularity globally due to their effectiveness, minimal invasiveness, and improved patient outcomes.
Rising Popularity Worldwide: As technology advances, laparoscopy and hysteroscopy have become the standard for treating a range of gynecological issues. Women across the world, from developed nations to emerging economies, have access to these life-changing treatments. Countries in Europe, North America, and Asia are seeing increased use of minimally invasive gynecology, with a growing number of hospitals and clinics offering these procedures.
How Technology Is Expanding Access: The advent of robotic surgery, advanced imaging techniques, and telemedicine has further expanded access to gynecological endoscopic procedures. These innovations not only increase precision but also help doctors in remote areas offer the benefits of laparoscopy and hysteroscopy.
Cultural Shift in Women's Health: In many cultures, there is now a greater focus on women’s health and the importance of early diagnosis and minimally invasive treatments. The global appeal of these procedures is part of a larger shift towards better healthcare outcomes and more options for women’s reproductive and pelvic health.
Advantages of Minimally Invasive Surgery
The main advantage of gynecological endoscopic procedures is that they are minimally invasive, which significantly reduces recovery time and complications.
Shorter Recovery Times: Most women can return to normal activities within 1 to 2 weeks after surgery, compared to 4-6 weeks for traditional surgeries.
Reduced Pain and Scarring: Small incisions mean less pain and scarring, making these procedures aesthetically and physically advantageous.
Lower Risk of Complications: With less tissue disruption, there’s a lower risk of infection, bleeding, and damage to surrounding organs.
These advantages make endoscopic procedures a preferred choice for many patients, as they provide quicker healing and a safer overall experience.
Common Side Effects and Risks
While gynecological endoscopic procedures are generally safe, they do come with some potential risks.
Infection: As with any surgery, there’s a slight risk of infection, though it is rare due to the small incisions used.
Bleeding: Some bleeding may occur during or after the procedure, particularly if the surgery involves the removal of large fibroids or other tissue.
Injury to Surrounding Organs: Though rare, there’s a slight chance of damaging surrounding organs such as the bladder, intestines, or blood vessels during surgery.
Patients are carefully monitored to minimize these risks, and with skilled surgeons, the likelihood of complications is very low.
Patient Education and Expectations
Before undergoing laparoscopy or hysteroscopy, it’s essential for patients to have realistic expectations about their procedure.
Pre-Surgery Preparation: Patients should follow the doctor’s instructions carefully, which may include fasting before surgery, stopping certain medications, or undergoing additional tests.
During the Procedure: Both laparoscopy and hysteroscopy are typically done under general anesthesia. The length of the surgery can vary, but most procedures are completed within 30 minutes to 2 hours.
Post-Surgery Care: After the procedure, most patients are advised to rest and limit physical activity for a few days. Any pain can usually be managed with over-the-counter pain relievers.
Proper education helps set realistic expectations and prepares patients for a smoother recovery.
Recovery After Gynecological Endoscopic Surgery
One of the greatest advantages of gynecological endoscopic surgeries is the fast recovery time compared to traditional open surgeries. The use of small incisions reduces the risk of infection, scarring, and the time it takes for the body to heal.
Recovery Time for Laparoscopy and Hysteroscopy: Most women can expect to return to their normal activities within 1 to 2 weeks after laparoscopy or hysteroscopy. The exact recovery time varies depending on the complexity of the procedure and the patient’s health, but it’s generally much shorter than traditional surgeries.
Post-Operative Care: After the procedure, patients may experience some discomfort, bloatedness, or mild cramping, but these symptoms typically subside within a few days. Pain management and rest are essential for a full recovery.
Risks and Complications: While complications are rare, infection, bleeding, or damage to surrounding organs can occur. These risks are significantly lower in laparoscopy and hysteroscopy than in open surgery, and careful monitoring by the healthcare provider helps ensure a smooth recovery.
Future of Gynecological Endoscopic Procedures
The future of gynecological endoscopic procedures looks bright, with continuous advancements in technology and techniques.
Robotic Surgery: Robotic-assisted laparoscopy is one of the most exciting developments. It offers enhanced precision, better visualization, and smaller incisions, which result in even shorter recovery times and fewer complications.
Enhanced Imaging: The use of advanced imaging technology, such as 3D laparoscopy, is improving diagnosis and treatment. These tools help surgeons visualize complex conditions more clearly, leading to more accurate treatments.
Global Accessibility: As medical technology becomes more widespread, gynecological endoscopic procedures are becoming more accessible, even in remote regions, allowing women worldwide to benefit from these treatments.
The continued evolution of these procedures promises even more effective, safer, and accessible treatments for women’s health in the future.
How to Choose the Right Surgeon for Endoscopic Procedures
Choosing the right surgeon for gynecological endoscopic procedures is crucial for a successful outcome.
Credentials and Experience: It’s essential to ensure that the surgeon has proper qualifications, such as board certification in gynecology or minimally invasive surgery. They should also have substantial experience with the specific procedure you're undergoing, whether it’s laparoscopy or hysteroscopy.
Patient Reviews and Referrals: Asking for referrals from trusted sources, like family or primary care physicians, can help guide your choice. Many patients also look at online reviews or testimonials for a better understanding of the surgeon’s approach.
Consultation: A good surgeon will take the time to explain the procedure, discuss potential risks, and answer any questions you might have. This consultation is crucial in determining if the surgeon is a good fit for your needs.
Choosing a qualified and experienced surgeon is one of the most important steps in ensuring the success of your gynecological endoscopic surgery.
The Impact on Women's Health and Well-being
Gynecological endoscopic procedures have a profound impact on women's health, often improving both their physical and emotional well-being.
Enhanced Quality of Life: By addressing conditions like fibroids, endometriosis, and abnormal bleeding, these procedures provide significant relief from symptoms that can impact a woman’s daily life. Women report a reduction in pain, improved fertility, and better overall health following surgery.
Emotional and Psychological Benefits: Many women find that gynecological endoscopic procedures positively affect their self-esteem and body image. The ability to have a less invasive procedure, with a quicker recovery and less visible scarring, helps many women feel more confident in their bodies.
Long-Term Health Benefits: Treating gynecological conditions with endoscopy can also prevent long-term complications, such as infertility or chronic pain, offering lasting improvements in health and quality of life.
These procedures offer not just physical health benefits, but emotional and psychological well-being, which is an important aspect of holistic healthcare.
Patient Testimonials and Case Studies
Real-life patient experiences offer invaluable insights into the outcomes of gynecological endoscopic procedures.
Case Study: Fibroid Treatment: One patient shared her experience with laparoscopic myomectomy to remove fibroids. After years of heavy bleeding and pain, the procedure relieved her symptoms. She was back to her regular activities in just two weeks, and her fertility improved significantly, allowing her to conceive naturally within a year.
Case Study: Endometriosis Relief: Another patient underwent laparoscopy to treat endometriosis. Previously struggling with painful periods and infertility, the surgery provided significant symptom relief, and within months, she was able to conceive.
Testimonial: A patient who had a hysteroscopic procedure for abnormal bleeding shared that she felt more confident and comfortable after the surgery. She described how the minimally invasive approach left her with little pain and no visible scarring, and the results drastically improved her quality of life.
Patient testimonials and case studies highlight the effectiveness and positive impact of these procedures, showing how they improve not only physical health but overall well-being.
Conclusion
Gynecological endoscopic procedures, including laparoscopy and hysteroscopy, have revolutionized the way many common gynecological conditions are treated. These minimally invasive techniques offer significant advantages over traditional surgery, such as quicker recovery times, reduced pain, and smaller scars. As a result, they have become the preferred option for diagnosing and treating conditions like fibroids, endometriosis, and abnormal uterine bleeding.
The benefits of these procedures extend beyond physical health. Many women experience emotional and psychological improvements after their surgeries, with increased confidence and enhanced quality of life. With advancements in surgical technology and techniques, the future of gynecological endoscopy looks even brighter, providing women worldwide with safe, effective, and accessible options for improving their health.
By choosing an experienced surgeon, understanding the risks and benefits, and setting realistic expectations, patients can ensure they are well-prepared for a successful outcome. Whether improving fertility, reducing pain, or enhancing overall well-being, gynecological endoscopic procedures are an essential tool in modern women’s healthcare.