What is IVF and How Does it Work?
In-Vitro Fertilization (IVF) is a popular assisted reproductive technology that helps individuals and couples struggling with infertility. It involves combining eggs and sperm outside the body in a laboratory setting, then transferring the resulting embryo(s) into the uterus. IVF is often recommended when other fertility treatments have been unsuccessful or when there are specific medical conditions that make natural conception difficult.
The IVF process starts with ovarian stimulation, where hormone injections are given to the woman to encourage her ovaries to produce multiple eggs. Once the eggs mature, they are retrieved from the ovaries. These eggs are then fertilized with sperm in the laboratory. The fertilized eggs, now embryos, are monitored for growth and development. The healthiest embryos are selected and transferred into the woman’s uterus for implantation.
IVF is a powerful tool in overcoming infertility, with its ability to bypass natural barriers to conception. However, it is a complex and emotionally challenging procedure that requires careful monitoring and support.
IVF Success Rates: What Affects Your Chances of Pregnancy?
IVF success rates vary widely, depending on several factors like age, fertility diagnosis, and the clinic's quality. On average, IVF success rates range from 40% to 50% for women under 35, with a decline in success as age increases. For women over 40, the success rate typically drops to around 10-20%.
Key factors influencing IVF success include:
Egg quality: As women age, egg quality decreases, affecting the chances of a successful pregnancy.
Embryo health: The quality of the embryo, which can be assessed through genetic screening or embryo grading, plays a significant role in implantation success.
Sperm quality: Healthy sperm is essential for fertilizing the egg and ensuring the embryo's viability.
Clinic experience: IVF success rates also vary by clinic. High-quality clinics with advanced technology and experienced staff tend to have better outcomes.
While IVF can significantly increase the chances of pregnancy, it is important for patients to manage expectations and understand the variables that affect success.
IVF Medications and Hormonal Injections
IVF treatment involves hormonal medications to stimulate the ovaries and support the development of multiple eggs. The primary medications include:
Gonadotropins (FSH, LH): These hormones stimulate the ovaries to produce several eggs rather than the single egg that naturally occurs during a regular cycle.
GnRH agonists or antagonists: Used to prevent premature ovulation and help control the timing of egg retrieval.
HCG (Human Chorionic Gonadotropin): This hormone triggers the final maturation of eggs before they are retrieved.
These medications are typically administered through daily injections, and their dosages are carefully monitored by the fertility clinic. While these medications are essential for the success of IVF, they can cause side effects like bloating, mood swings, and ovarian hyperstimulation syndrome (OHSS) in some cases.
Patients undergoing IVF are closely monitored through blood tests and ultrasounds to track the response to the medications and adjust doses as necessary. Though these injections can be uncomfortable, they play a crucial role in preparing the body for IVF.
The IVF Process Timeline: What to Expect
The IVF process typically spans several weeks, from initial consultation to pregnancy test. Here’s a basic timeline:
Ovarian Stimulation (10-14 days): Hormonal injections are given to stimulate the ovaries to produce multiple eggs. This period is closely monitored with blood tests and ultrasounds.
Egg Retrieval (1 day): When the eggs are ready, they are retrieved under light anesthesia. This outpatient procedure usually takes about 20 minutes.
Fertilization and Embryo Culture (3-5 days): Eggs are fertilized in the lab, and the embryos are cultured for a few days. Some may undergo genetic screening to ensure quality.
Embryo Transfer (3-5 days after retrieval): One or more healthy embryos are selected and transferred into the uterus.
Pregnancy Test (10-12 days after transfer): A blood test confirms if the embryo has implanted successfully. If positive, follow-up ultrasounds are done.
Though IVF is structured, timing can vary slightly depending on how the body responds to medication.
IVF Costs: What Should You Expect to Pay?
IVF can be an expensive process, with costs varying widely depending on location, clinic, and additional treatments needed (like egg donation or genetic screening). On average, a single IVF cycle can cost between $10,000 and $15,000 in countries like the United States. Additional costs for medications, consultations, and embryo freezing can push the total closer to $20,000 or more.
Some countries offer more affordable IVF options:
India: IVF costs can be as low as $2,000 to $4,000 per cycle, making it a popular destination for medical tourism.
Mexico: Costs for IVF in Mexico range from $5,000 to $7,000, with several renowned clinics catering to international patients.
Eastern Europe: Countries like the Czech Republic and Greece offer IVF services at a lower cost than Western Europe, typically around $5,000 to $7,500 per cycle.
Insurance coverage for IVF varies, and many insurance policies do not fully cover the procedure. Some clinics offer financing plans or payment options to help manage the costs.
IVF for Women Over 40: Challenges and Considerations
For women over 40, IVF can be an effective treatment, though it presents certain challenges. As a woman ages, egg quality and quantity decline, leading to lower IVF success rates. Women in this age group may face higher risks of miscarriage and chromosomal abnormalities.
However, IVF still offers hope:
Egg Donation: Many women over 40 opt for egg donation, which can significantly improve success rates as donated eggs are often from younger women.
Pre-implantation Genetic Testing (PGT): This technology screens embryos for genetic abnormalities, which is especially helpful for women over 40.
The IVF process for older women requires more careful monitoring and may involve additional treatments or screening to maximize the chances of a successful pregnancy.
IVF with Egg Donation: A Viable Option for Some Patients
Egg donation is a common option for women who cannot use their own eggs due to age, poor egg quality, or medical conditions. In this process, eggs from a donor are fertilized with the male partner’s sperm (or donor sperm) and the resulting embryos are transferred to the recipient’s uterus.
Key points about egg donation:
Donor Selection: Egg donors are carefully selected based on health, genetic history, and other factors.
Success Rates: IVF with egg donation generally has higher success rates than using a woman’s own eggs, especially for those over 40.
Legal and Ethical Considerations: The legalities surrounding egg donation vary by country, including donor anonymity, parental rights, and compensation.
Egg donation offers a successful path to parenthood for many women facing fertility challenges.
IVF and Male Infertility: Overcoming Male Factor Issues
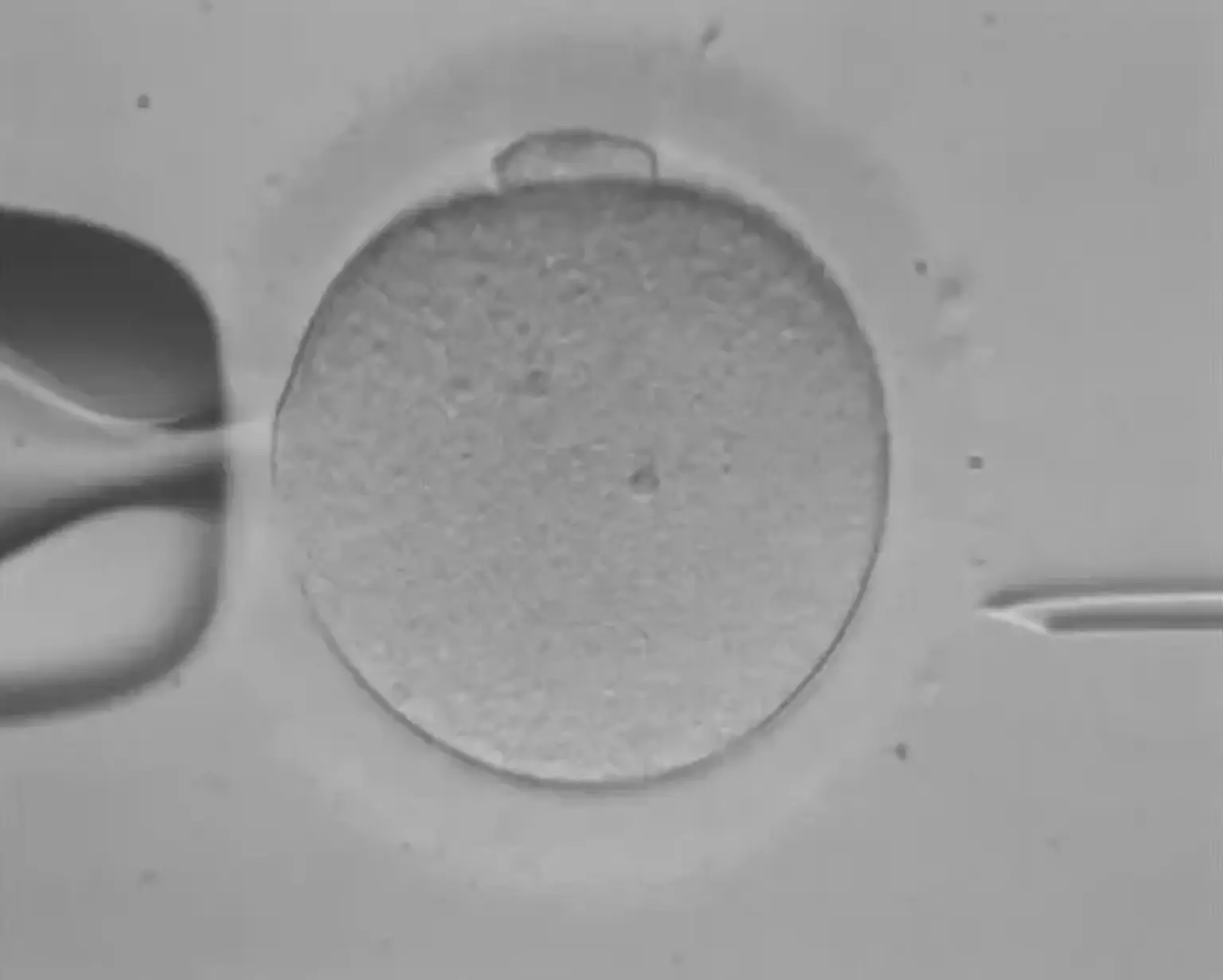
Male infertility accounts for about 30-40% of fertility problems. For couples struggling with male infertility, IVF combined with ICSI (Intracytoplasmic Sperm Injection) offers a solution. ICSI involves injecting a single sperm directly into an egg to achieve fertilization, bypassing issues like low sperm count, poor motility, or abnormal sperm shape.
Other options for male infertility include:
Sperm Retrieval: In cases where sperm is absent in semen, it can be surgically retrieved directly from the testes or epididymis.
Sperm Donor: For severe male infertility, donor sperm may be used in conjunction with IVF.
IVF with ICSI allows men with various fertility issues to father children, providing a much-needed option when natural conception is not possible.
IVF and Embryo Freezing: A Popular Fertility Preservation Option
Embryo freezing (or cryopreservation) is an essential part of the IVF process, particularly for those who want to preserve fertility for future use. After an IVF cycle, excess healthy embryos may be frozen and stored for later use. This option is particularly useful for women who are undergoing IVF at a young age and wish to delay pregnancy until later in life.
Embryo Storage: Frozen embryos can be stored for several years, offering flexibility and options for future pregnancies.
Success Rates: Frozen embryo transfers have similar success rates to fresh transfers, with some studies suggesting a slight advantage due to more careful selection of embryos.
Cost: Storing embryos incurs additional fees, but it provides an opportunity for future pregnancies without repeating the IVF process.
Embryo freezing offers individuals more control over their reproductive timelines, especially those with health or age-related concerns.
IVF with Surrogacy: A Solution for Families Who Cannot Carry a Pregnancy
For some couples, carrying a pregnancy is not an option due to medical conditions, such as uterine abnormalities, or if the woman is unable to carry a pregnancy to term. In these cases, IVF with surrogacy offers a potential solution.
Surrogacy involves a woman (the surrogate) carrying the pregnancy on behalf of the intended parents. There are two types of surrogacy:
Traditional Surrogacy: The surrogate is also the biological mother of the child, as her eggs are used.
Gestational Surrogacy: The surrogate carries an embryo created from the eggs and sperm of the intended parents or donors. The surrogate has no genetic connection to the baby.
While surrogacy can be a life-changing option, it involves legal, ethical, and emotional complexities. Intended parents should be prepared for the financial and emotional investment, as well as the legal arrangements.
The Role of IVF Clinics: How to Choose the Right One
Choosing the right IVF clinic is crucial for a successful outcome. Several factors should be considered when selecting a clinic:
Success Rates: Research the clinic's IVF success rates, especially for your specific age group and fertility condition.
Reputation and Reviews: Look for patient testimonials and reviews about the clinic’s services, facilities, and customer care.
Clinic Facilities: A state-of-the-art lab with the latest technology can improve your chances of success. Ask about their equipment, laboratory procedures, and embryo culture systems.
Consultation Process: The clinic should offer personalized care with a thorough consultation to assess your fertility needs and provide clear communication about costs, risks, and expectations.
The right clinic can make a big difference in IVF outcomes, so it’s important to do thorough research and feel comfortable with the team.
IVF and Lifestyle Factors: How to Improve Your Chances of Success
Your lifestyle choices can play a significant role in the success of IVF treatment. Factors such as diet, exercise, smoking, and alcohol consumption can impact fertility and the outcome of IVF. Here are some lifestyle changes that may improve your chances:
Maintain a Healthy Weight: Both underweight and overweight women may experience reduced fertility. A balanced diet and regular exercise can help achieve a healthy body mass index (BMI).
Quit Smoking: Smoking damages eggs and sperm and increases the risk of miscarriage, premature birth, and low birth weight.
Limit Alcohol and Caffeine: Excessive alcohol and caffeine consumption can negatively impact fertility and IVF success. Moderation is key.
Stress Management: High stress levels can affect hormone production and overall fertility. Practices like yoga, meditation, or deep breathing exercises may help reduce stress.
By making healthy lifestyle changes, patients can potentially enhance their IVF success rates and overall reproductive health.
Risks and Complications of IVF: What You Need to Know
Like any medical procedure, IVF carries potential risks and complications:
Ovarian Hyperstimulation Syndrome (OHSS): Caused by an overreaction to fertility drugs, OHSS can lead to swollen ovaries, abdominal pain, and, in rare cases, serious complications.
Multiple Pregnancies: IVF increases the chance of twins or triplets if multiple embryos are transferred, which can carry higher health risks for both the mother and babies.
Ectopic Pregnancy: Though rare, an embryo can implant outside the uterus, typically in the fallopian tube, requiring medical intervention.
Emotional Strain: IVF can be emotionally and financially draining, especially if multiple cycles are needed or the outcome is unsuccessful.
IVF clinics take extensive precautions to minimize risks and monitor patients closely throughout the process. Discussing these risks upfront with your fertility specialist will help you make an informed decision.
The Emotional Journey of IVF: Coping with the Highs and Lows
IVF is not just a physical process; it’s also an emotional one. The rollercoaster of hope, anxiety, and disappointment can take a toll on individuals and couples. It’s essential to be prepared for the emotional challenges of IVF:
Stress and Anxiety: The uncertainty of the outcome and the financial and physical commitment can cause significant stress. Managing expectations and seeking emotional support can help.
Grief and Disappointment: If IVF doesn’t result in a pregnancy, feelings of loss are common. It’s crucial to give yourself permission to grieve and seek help if needed.
Support Systems: Talking with a partner, friends, or a therapist can provide emotional relief. Joining support groups with others going through IVF can also offer a sense of community.
Having a strong support system and focusing on mental well-being can make the IVF journey more manageable and emotionally fulfilling.
IVF and Global Trends: Where is IVF Most Popular?
IVF has become a widely accepted fertility treatment worldwide, with varying levels of access, cost, and success rates across different countries. Here are some key trends:
United States: IVF is highly advanced and widely available, but the costs can be prohibitive for many. Insurance coverage is inconsistent, often leaving patients to pay out-of-pocket.
Europe: Countries like Spain, the Czech Republic, and Greece offer high-quality IVF services at more affordable prices, attracting many medical tourists.
Asia: In countries like India and Thailand, IVF treatments are offered at lower costs, drawing patients from around the world. Clinics in these regions are known for providing high-quality care at a fraction of the price.
Australia: IVF is accessible and highly regulated, ensuring that patients receive safe and effective treatment, though costs are rising.
The popularity of IVF is increasing globally, and patients often seek options that balance quality care with cost efficiency, sometimes opting for medical tourism to access more affordable treatments.
Future Advances in IVF: What’s Next for Fertility Treatment?
The field of IVF continues to evolve, with new technologies and advancements improving success rates and making treatment more accessible. Some of the most promising developments include:
Genetic Screening: Pre-implantation genetic testing (PGT) helps identify genetic abnormalities in embryos, increasing the likelihood of a healthy pregnancy.
Stem Cell Research: Stem cell therapy holds potential for creating eggs and sperm from other cell types, potentially bypassing infertility altogether.
Artificial Intelligence: AI is being used to analyze embryo development, making embryo selection more accurate and improving success rates.
Improved Cryopreservation: Advances in freezing techniques are allowing embryos, eggs, and sperm to be preserved with better survival rates, offering more options for fertility preservation.
As science continues to progress, IVF treatments are expected to become more efficient, less invasive, and more widely accessible, offering hope to even more individuals and couples facing infertility.
IVF and the Role of Genetics: Enhancing Success Rates
Genetics play a crucial role in IVF outcomes, as genetic abnormalities can impact embryo development and implantation. To address this, advancements in genetic testing, such as Preimplantation Genetic Testing (PGT), have been introduced. PGT allows doctors to screen embryos for genetic conditions like Down syndrome, cystic fibrosis, and other inherited disorders before implantation.
PGT-A: Screens for chromosomal abnormalities, which are common in older women.
PGT-M: Tests for specific genetic diseases.
PGT-SR: Identifies structural rearrangements of chromosomes.
Genetic testing helps identify the healthiest embryos, increasing the likelihood of a successful pregnancy and reducing the risk of miscarriage.
IVF and Sperm Selection: The Role of ICSI
In cases of male infertility, Intracytoplasmic Sperm Injection (ICSI) is a procedure used alongside IVF to increase fertilization chances. ICSI involves injecting a single sperm directly into an egg, bypassing issues like low sperm count, poor motility, or abnormal sperm morphology.
ICSI has revolutionized the treatment of male infertility by making IVF an option for men with severe sperm issues. It significantly improves fertilization rates and is often recommended when conventional insemination methods fail.
IVF and the Risk of Multiple Pregnancies
One of the risks of IVF is multiple pregnancies (twins, triplets, or more), which can arise when more than one embryo is transferred. Multiple pregnancies carry higher risks for both mother and babies, including:
Premature birth: Multiple pregnancies are more likely to result in preterm labor.
Low birth weight: Babies born prematurely are often underweight and may face health challenges.
Health complications: The mother may face increased risk of gestational diabetes, preeclampsia, and other pregnancy-related issues.
To reduce the risks, many clinics now practice single embryo transfer (SET), where only one healthy embryo is transferred to the uterus, lowering the chance of multiples.
IVF After Failed Cycles: What Are Your Options?
It’s common for IVF to require multiple cycles to achieve a successful pregnancy. If an IVF cycle fails, patients often feel discouraged, but there are options for moving forward:
Reviewing the Cause: Doctors will evaluate why IVF failed, which could be due to embryo quality, hormonal imbalances, or uterine issues.
Adjusting the Treatment Plan: Changes may include altering medications, trying a different stimulation protocol, or using egg or sperm donors.
Embryo Freezing: If some embryos remain viable after a failed cycle, frozen embryos can be used for future attempts.
Consider a Surrogate: If there are issues with the uterus or implantation, gestational surrogacy may be an option.
While it’s emotionally challenging, many patients find success after one or more IVF cycles, with doctors adjusting the approach based on previous outcomes.
Conclusion
IVF has transformed the landscape of fertility treatment, offering hope to individuals and couples facing infertility. While it involves physical, emotional, and financial challenges, the advancements in technology, genetics, and personalized care have significantly improved success rates. From egg donation and surrogacy to genetic screening and ICSI, IVF presents various options tailored to individual needs.
Choosing the right clinic, maintaining a healthy lifestyle, and managing expectations are essential steps in this journey. Though IVF can take time and patience, for many, it ultimately leads to the fulfilling experience of parenthood. With ongoing advancements, the future of IVF is brighter than ever, offering new possibilities for families worldwide.