Intensity-modulated Radiation Therapy (IMRT)
Overview
Cancer is caused by uncontrolled cell growth. As the number of cells increases, a mass or tumor forms. Cancer cells, which comprise the tumor, multiply rapidly. When normal, healthy cells come into contact with other cells, they cease reproducing and developing. Cancer cells, on the other hand, do not and continue to develop. Radiation treatment causes DNA damage in cells by using high-energy x-rays. This either destroys the cancer cells or prevents them from replicating. External radiation and internal radiation are the two basic forms of radiation treatment.
What is Intensity-Modulated Radiation Therapy (IMRT)?
A radiation beam is sent into the body during external radiation treatment. intensity-modulated radiation treatment (IMRT) is a form of external beam radiation. IMRT is a popular method of delivering radiation treatment for various forms of cancer.
Radiation treatment, including IMRT, destroys the DNA and prevents cancer cells from reproducing and developing, resulting in tumor development that is slowed or stopped. Radiation treatment is capable of destroying all cancer cells in many situations, reducing or eradicating tumors. Radiation treatment may be used with surgery (adjuvant radiation). After surgery, radiation is used to target possible microscopic disease in this circumstance.
Intensity-modulated radiation treatment (IMRT) is a high-precision radiotherapy technique that use computer-controlled linear accelerators to deliver exact radiation doses to a malignant tumor or particular locations inside the tumor. By modulating or controlling the intensity of the radiation beam in many tiny compartments, IMRT allows the radiation dosage to adapt more accurately to the three-dimensional (3-D) structure of the tumor. IMRT also enables for larger radiation doses to be targeted on the tumor while reducing the dosage to normal essential structures surrounding it.
Treatment is meticulously prepared by combining 3-D computed tomography (CT) or magnetic resonance imaging (MRI) pictures of the patient with computerized dose calculations to determine the radiation intensity pattern that best conforms to the tumor shape. Combinations of numerous intensity-modulated fields originating from distinct beam directions often result in a personalized radiation dosage that enhances tumor exposure while limiting damage to nearby normal tissues.
Because the IMRT strategy reduces the normal tissue dose to tumor dose ratio to a minimum, larger and more effective radiation doses may be administered to tumors safely and with fewer side effects than conventional radiotherapy treatments. Even when dosages are not raised, IMRT has the potential to lessen treatment toxicity. When compared to conventional radiation, IMRT requires somewhat longer daily treatment periods as well as additional planning and safety tests before the patient may begin treatment.
What are the benefits of IMRT?
By altering and modulating the radiation beam into numerous smaller beams, IMRT permits the radiation dosage to fit more accurately to the three-dimensional structure of the tumor. This allows for a larger dosage of radiation to be administered to the tumor while preserving healthy tissue in the surrounding area. The machine molds the radiation into changing shapes throughout the therapy to deliver these smaller beams.
Who will be involved in this procedure?
For IMRT distribution, most facilities rely on professionally trained personnel. The radiation oncologist, medical physicist, dosimetrist, radiation therapist, and radiation therapy nurse are all members of this team.
The radiation oncologist, a specially educated physician, initially meets with the patient to evaluate if IMRT is the best treatment option. The specific course of therapy is planned after gaining informed permission.
A radiation physicist with specific expertise in medical physics guarantees that the linear accelerator provides the proper radiation dosage and that computerized dose estimates are correct. A dosimetrist collaborates with a medical physicist to create the IMRT plan and beam configurations required to provide the radiation oncologist's dosage.
The final treatment plan is validated on the treatment machine by a medical physicist using a phantom (a device that resembles the human body) that monitors the dosage supplied by the treatment plan. This guarantees that the radiation oncologist's planned dosage is given by the machine. The patient is placed on the treatment table and the machine is operated by a radiation therapist.
During treatment, the oncology nurse checks the patient and offers more information regarding the treatment and any side effects. In consultation with the physician, the radiation oncology nurse also assists in the management of any responses or side effects from therapy that may develop.
When is IMRT used?
Prostate cancer, head and neck cancers, gastrointestinal and gynecologic cancers, lung cancers, and brain tumors are all treated with IMRT.
When a tumor partially surrounds or is very close to a healthy part of your body that cannot tolerate the full dose of radiation being given to the tumor, IMRT is commonly used. When the tumor is not in close proximity to sensitive regions, IMRT may not be required. For example, surface tumors may not respond well to IMRT but may respond to other forms of radiation. Consult with your radiation team to determine which treatment option is best for you.
IMRT provides for the precise delivery of treatment to strangely shaped tumors and may also produce concave (hollow) regions inside the high dose region radiation therapy. This reduces the dose of radiation sent to a sensitive organ, such as the rectum (lower colon) or the spinal cord. Cancers in regions of the body that were previously unsafe to treat with radiation treatment can now be treated using IMRT. Most tumor types are currently treated using IMRT.
Specific examples include:
- Brain tumors – IMRT may allow for a reduction in the radiation to the eyes and other key regions of the brain, so preventing harm. The dosage to hormone-producing parts of the brain, as well as memory centres, can be lowered.
- Head, neck and face cancers – IMRT can dramatically lower the dosage to the salivary glands, hence minimizing one of the most serious long-term adverse effects of treating some of these tumors in the past - dry mouth (xerostomia).
- Breast and lung cancers – To minimize dosages to the heart and lungs, IMRT can be employed. IMRT has been found to minimize skin responses after breast cancer therapy. If the tumor is close to the spine, IMRT can provide a larger dosage without harming the spinal cord. Because spinal cord injury is one of the most dangerous uncommon adverse effects of radiation, therapy close to the spinal cord was frequently avoided or the dose was lowered in the past (causing paralysis or weakness). The danger of this is quite minimal with IMRT procedures.
- Abdominal and pelvic cancers – IMRT can be particularly helpful in decreasing side effects from cancer treatment in the stomach, pancreas, and lower esophagus. Radiation therapy for bowel malignancies (colorectal cancers) in the pelvis frequently employs IMRT to lessen the risk of bowel and bladder damage.
- Prostate cancer – IMRT is currently conventional treatment for localized prostate tumors, and it is frequently utilized following a surgery in which the cancer cells were not completely eradicated (radical prostatectomy). IMRT enables for greater doses to be delivered to the prostate, increasing the likelihood of cancer control (cure). It also implies that the lymph nodes may be treated more simply and with fewer adverse effects than previously. The rectum is the key organ proximal to the prostate that occasionally limits the dosage that may be safely administered (lower bowel). The quantity of rectum in the high dosage region can be reduced using IMRT. This implies that both short and long-term adverse effects have become far less prevalent.
- Cervix and uterine (endometrial or womb) cancer – IMRT is widely used to treat cancer that has or does not have pelvic lymph nodes. Again, IMRT improves precision while decreasing short-term and late effects, mostly related to bladder and intestinal irradiation.
The only possible downside for patients receiving IMRT may be a little longer treatment time - but this is still only a few minutes each session, depending on the conditions. Other IMRT methods, such as VMAT (volumetric modulated arc therapy), have the potential to shorten treatment duration. Because of the modest radiation doses supplied to tissues around the malignancy, IMRT may result in a higher total body tissue dosage (integral dose). This is especially important for young patients.
Is IMRT right for me?
Although IMRT can be helpful, it is not always the best option for patients. Because the radiation beams are arranged in various angles around the patient, a low dosage 'bath' of radiation is produced just outside the tumor. It is unknown if this low-dose zone creates problems, but your radiation team will constantly strive to reduce radiation exposure to normal tissue. Depending on which organs are inside this low-dose area, spreading out low-dose radiation may produce immediate or late radiation adverse effects.
IMRT can potentially result in radiation "hot spots" or "cold areas." Hotspots in organs can increase the patient's risk of side effects, while cold areas can indicate that the tumor is not receiving enough radiation dosage to control the malignancy.
Planning and administering an IMRT treatment take longer than other types of radiation therapy. As with other radiation treatments, patients must be able to remain pleasantly still (immobilized) throughout the duration of the therapy. Even minor movements by the patient during treatment might have an impact on how well IMRT works.
To cure cancer or control symptoms, medicine must sometimes be administered rapidly. Because of discomfort or movement concerns, some patients may be unable to remain motionless during radiotherapy. IMRT would not be the best solution in these circumstances.
What equipment is used?
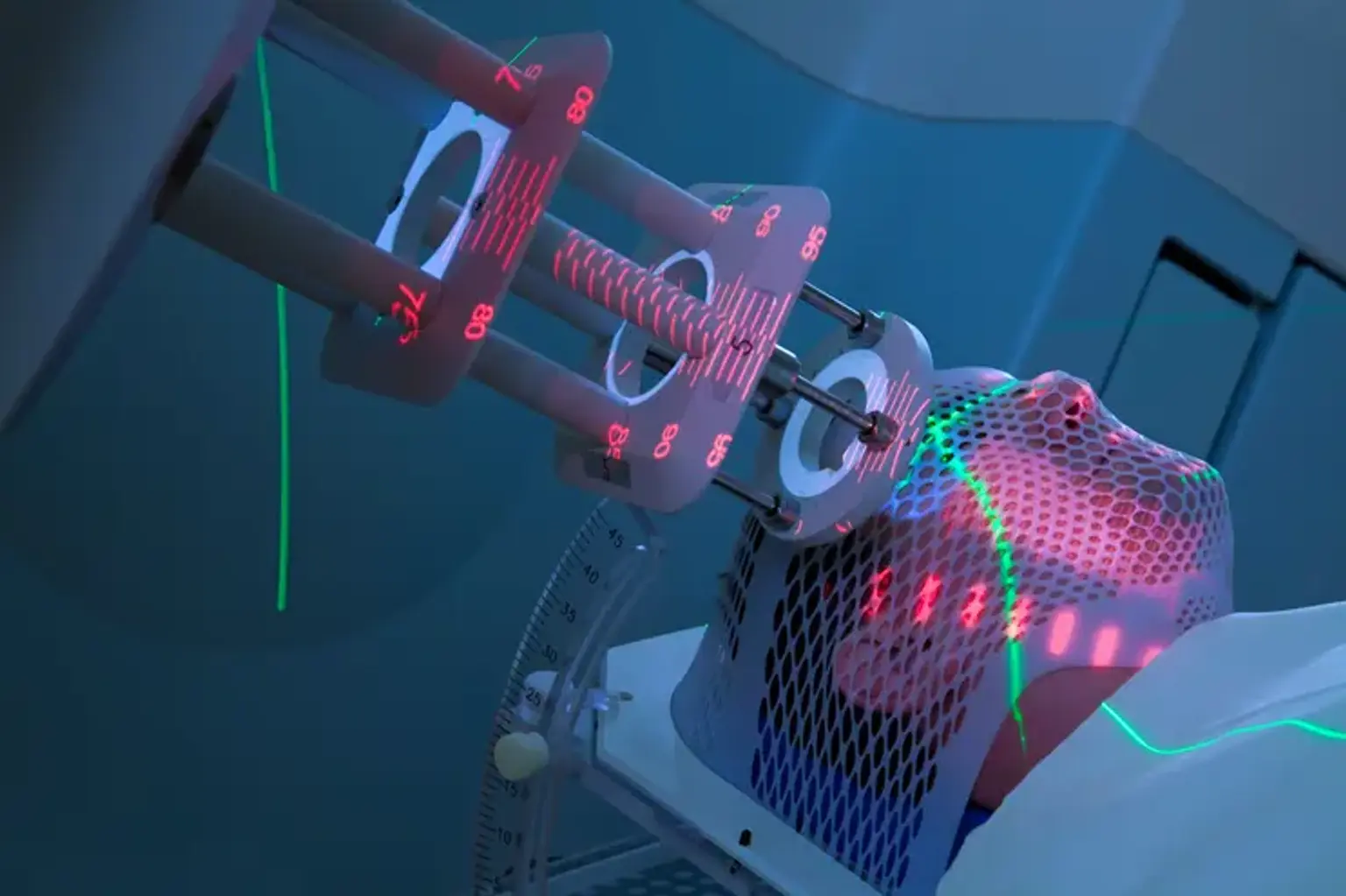
The photons, or x-rays, utilized in IMRT are generated by a medical linear accelerator (LINAC). The machine is about the size of a compact vehicle, standing around 10 feet tall and 15 feet long. The patient must remain motionless during the therapy. Depending on the treatment plan, the strength of each beam's radiation dosage is dynamically changed. While the radiation is on, the patient will not feel anything, but will hear noise from the machine, smell an odor from the electronic equipment, or see the danger signal light.
The machine's sounds and scents are typical. During treatment, the patient is alone in the room but is continually observed by radiation therapists from outside the room. The time spent in the treatment room varies depending on the plan, but it is normally between 15 minutes and one hour.
Is there any special preparation needed for the procedure?
A physical examination and medical history review will be performed prior to treatment planning. Following that, there is a treatment simulation session that involves CT scans. To assist orient and target the equipment, a tiny mark or tattoo may be put on the patient's skin. This scan is used by the radiation oncologist to create a personalized treatment plan for the patient. In certain situations, a mask or other device will be created to keep the patient immobile during treatment. Prior to the simulation and therapy, the patient may be told to follow a specific bowel and bladder preparation routine or too fast. During the CT scan, intravenous contrast material may be administered to assist clarify the tumor.
Additional scanning modalities, such as positron emission tomography (PET) and magnetic resonance imaging (MRI), may be necessary for IMRT planning on occasion. These diagnostic pictures can be used with the planned CT to assist the radiation oncologist in pinpointing the exact position of the tumor target.
In other circumstances, radio dense markers must be inserted inside the target for more exact location. IMRT treatments often begin a week or two following simulation.
How is the procedure performed?
Multiple (fractionated) treatment sessions on separate days are frequently required with IMRT. To determine the number of treatments, the radiation oncologist examines the kind, location, and size of the tumor, doses to normal structures, and the patient's health. Patients are typically scheduled for IMRT treatments five days a week for five to eight weeks.
The radiation therapist sets the patient on the treatment table at the start of the treatment session, guided by the markings on the skin (tattoos) outlining the treatment region. If molded devices were created, they will be employed to assist the patient in maintaining the correct posture. During the process, the patient may be moved. To check placement and marker location, imaging equipment on the treatment machine such as x-ray or CT may be employed. Treatment sessions are typically between 15 and 60 minutes long.
What will I feel during and after this procedure?
IMRT treatments, like other external beam radiation therapy treatments, are not supposed to be painful. However, if a patient develops discomfort as a result of the treatment position or positioning devices, the machine can be turned off. Some individuals may have therapy-related adverse effects as their treatment advances. The type of the side effects is determined by the normal tissue structures that are irradiated near the tumor. The radiation oncologist and the nurse will go through potential side effects and how to manage them.
Radiation therapy can have unintended consequences. These issues might be caused by the treatment itself or by radiation damage to healthy cells in the treated region. The frequency and severity of adverse effects will vary depending on the type of radiation used, the dose, and the body area being treated. Inform your doctor and/or nurse so that they can assist you in managing them.
Radiation can have both immediate and delayed negative effects. Early side effects occur during or immediately following therapy. They usually vanish within a few weeks. Fatigue and skin issues are common early adverse effects. The treatment area's skin may become sensitive, red, irritated, or swollen. Dryness, itching, peeling, and blistering are some of the other alterations.
Depending on the area being treated, other early side effects may include:
- Hair loss in the treatment area
- Mouth problems and difficulty swallowing
- Eating and digestion problems
- Diarrhea
- Nausea and vomiting
- Headaches
- Soreness and swelling in the treatment area
- Urinary and bladder changes
Late side effects may occur months or years following treatment. While they are often permanent, they are rare. They include:
- Brain changes
- Spinal cord changes
- Lung changes
- Kidney changes
- Colon and rectal changes
- Infertility
- Joint changes
- Lymphedema
- Mouth changes
- Secondary cancer
Radiation treatment carries a small chance of acquiring cancer. After treatment, your radiation oncologist will monitor for problems and recurring or new malignancies on a regular basis.
Radiation oncologists use procedures like IMRT to optimize radiation treatment's cancer-destroying potential while reducing its negative effects on healthy tissues and organs.
Conclusion
One of the most significant recent advancements in cancer is intensity-modulated radiation (IMRT). It allows for exact radiation dosage conformity to the target volume. It has the potential to minimize long-term morbidity and enhance local control dramatically. It enables cancer patients to get greater, more effective radiation doses while reducing harm to healthy tissues and organs surrounding them. This improves your chances of a cure while decreasing the possibility of negative effects.