Laparoscopic Cholecystectomy
What is laparoscopic cholecystectomy?
A cholecystectomy is a surgical procedure that removes your gallbladder, which is a pear-shaped organ located on the upper right side of your belly directly below your liver. The gallbladder collects and stores bile, which is a digestive fluid generated by the liver.
Laparoscopic cholecystectomy is a standard surgical procedure with a low risk of complications. You may usually go home the same day as your cholecystectomy. An open cholecystectomy is more intrusive than a laparoscopic cholecystectomy. This method of gallbladder removal requires a bigger incision.
A laparoscopic cholecystectomy is gallbladder removal operation. On the right side of your abdomen, the surgeon makes a few tiny incisions (belly). A laparoscope, a narrow tube with a camera on the end, is inserted through one incision by the surgeon. A screen displays your gallbladder. The gallbladder is subsequently removed through another tiny incision.
Laparoscopic cholecystectomy is a type of minimally invasive gallbladder removal operation. It is beneficial when gallstones cause inflammation, pain, or infection. The operation requires only a few minor incisions, and most patients are able to go home the same day and resume their daily activities. If you have any issues following surgery, contact your healthcare practitioner.
What are the indications for laparoscopic cholecystectomy?
Gallbladder stones (gallstones) are crystals that develop in the gallbladder. They can obstruct the passage of bile from the gallbladder into the digestive tract. Cholecystitis is caused by this blockage (inflammation of the gallbladder). Gallstones can also spread to other places of the body and create complications. A laparoscopic cholecystectomy treats gallstones that cause pain and infection.
Symptoms of gallstones include:
- Feeling bloated.
- Fever.
- Jaundice (yellow-looking skin).
- Nausea.
- Pain in the right side of the abdomen, which may reach the back or the shoulder.
Laparoscopic cholecystectomy has mainly replaced open cholecystectomies since the early 1990s. Current indications for laparoscopic cholecystectomy include acute or chronic cholecystitis, symptomatic cholelithiasis (gallstones), biliary dyskinesia, acalculous cholecystitis, gallstone pancreatitis, and gallbladder tumors or polyps. These are the same reasons for an open cholecystectomy. Gallbladder cancer is generally treated with open cholecystectomy.
What is the mechanism of gallbladder disease?
Gallbladder disease is caused by a malfunctioning gallbladder with the subsequent buildup of super-concentrated bile. The gallbladder normally releases its contents in response to physiologic changes caused by digestion (cholecystokinin hormone, vagal nerve stimulation, migrating myoelectric complex).
High cholesterol concentrations in the gallbladder are a recognized cause of the formation of cholesterol gallstones. Pigmented stones form as a result of hemolytic disorders (black stones) or infections (brown stones), where bacterial enzymes degrade bilirubin (bile component) into an insoluble form.
Stone formation is increased by stasis in the gallbladder or bile ducts. The cystic duct (the duct that drains the gallbladder) blockage is one example of gallbladder disease. Patients may have acute blockage of the cystic duct by stones, or they may experience acute acalculous cholecystitis, in which there is no mechanical obstruction but a functional obstruction, in the majority of severely sick patients. This blockage, whether mechanical or not, along with attempted bile excretion for digestion will result in acute gallbladder inflammation and pain (biliary colic).
Epidemiology of gallstone disease and laparoscopic cholecystectomy
Gallstones affect around 20 million people in the United States. Every year, roughly 300,000 cholecystectomies are done on this population. Asymptomatic gallstones affect 10% to 15% of the population. 20% of these are symptomatic (biliary colic). Approximately 1% to 4% of the 20% who are symptomatic will have problems such as, acute cholecystitis, gallstone pancreatitis, choledocholithiasis (bile duct stones), and gallstone ileus (bowel obstruction by stone).
Gallstones become increasingly common with age, with females being more prone than males to get gallstones. Gallstones affect roughly 20% of women and 5% of males between the ages of 50 and 65. Gallstones are made of cholesterol in 75% of cases, with the remaining 25% being pigmented. The clinical indications and symptoms are the same regardless of the type of gallstones.
Right upper quadrant or epigastric abdominal discomfort is a common symptom of gallbladder disease. The discomfort usually starts 30 minutes to two hours after eating fatty meals. The agony might endure anywhere from one to two hours to more than 24 hours. A subsequent infection known as acute cholecystitis is linked with pain that lasts longer than 24 hours. Due to sympathetic innervation, pain extends from the right upper quadrant to the right flank and, on rare occasions, to the right shoulder.
Nausea, bilious vomiting (containing bile), fever, chills, and diarrhea are some of the symptoms that may occur. Indigestion, GERD-like symptoms, Peptic Ulcer Disease symptoms, and dyspepsia are examples of less common symptoms. Pain will be intermittent and related to oral intake of fatty foods earlier in the illness phase. Pain may become more frequent and occur regardless of oral intake as the condition deteriorates.
How should I prepare for laparoscopic cholecystectomy?
Before the procedure, your healthcare team will perform a complete thorough history and physical examination, including abdominal examination, and specifically check for a “Murphy’s Sign.” (Deep palpation in the right upper quadrant while the patient inspires deeply. A positive test is when the patient abruptly stops their inspiration secondary to pain).
They will also discuss:
- Any drugs you are taking.
- Your options for pain management during and after surgery.
- Your surgeon may recommend fasting for a few hours before the surgery.
Laboratory tests:
CBC with differential (to test for increased white blood cells), Liver function panel (elevated bilirubin, alkaline phosphatase), Amylase/Lipase (pancreatic enzymes when are elevated can indicate gallstone pancreatitis).
Imaging studies that can be used:
- Abdominal ultrasound. Abdominal ultrasound of the right upper quadrant will detect the presence of gallstones, sludge, polyps, or masses, the thickness of the gallbladder wall (normally less than 3 mm), the width of the common bile duct (normally less than 6 mm, but 1 mm may be added per decade of life after 50 years of age or in pregnant women), and the presence/absence of fluid around the gallbladder.
- Magnetic resonance cholangiopancreatography (MRCP). MRI imaging research for noninvasive biliary and pancreatic duct visualization.
- Endoscopic Retrograde Cholangiopancreatography (ERCP). The biliary and pancreatic ducts are seen using x-rays and dye during an invasive endoscopic operation. ERCP has the benefit of being both diagnostic and therapeutic. This, however, is an intrusive operation with procedural hazards.
- Hepatobiliary Iminodiacetic Acid (HIDA) Scan. Imaging examination of the liver, gallbladder, and bile ducts. A radioactive tracer is delivered into the vein, where it binds to bile substrates before being digested by the liver. A nuclear scanner then follows the tracer's path through the liver, bile ducts, gallbladder, and duodenum. A measured ejection fraction of less than 35% generally indicates a clogged gallbladder. The reproduction of symptoms with cholecystokinin treatment has also been demonstrated to predict the remission of symptoms following cholecystectomy. Cholecystokinin should not be used in the presence of gallstones since it may cause the stones to flow into the common bile duct.
Pre-procedural anesthesia:
You will be sedated and pain-free during the procedure thanks to general anesthesia. Once you're asleep, your healthcare experts will insert a tube down your throat to assist you with breathing. They'll insert another tube, known as an IV line (catheter), into your arm to give fluids and drugs.
How laparoscopic cholecystectomy is done?
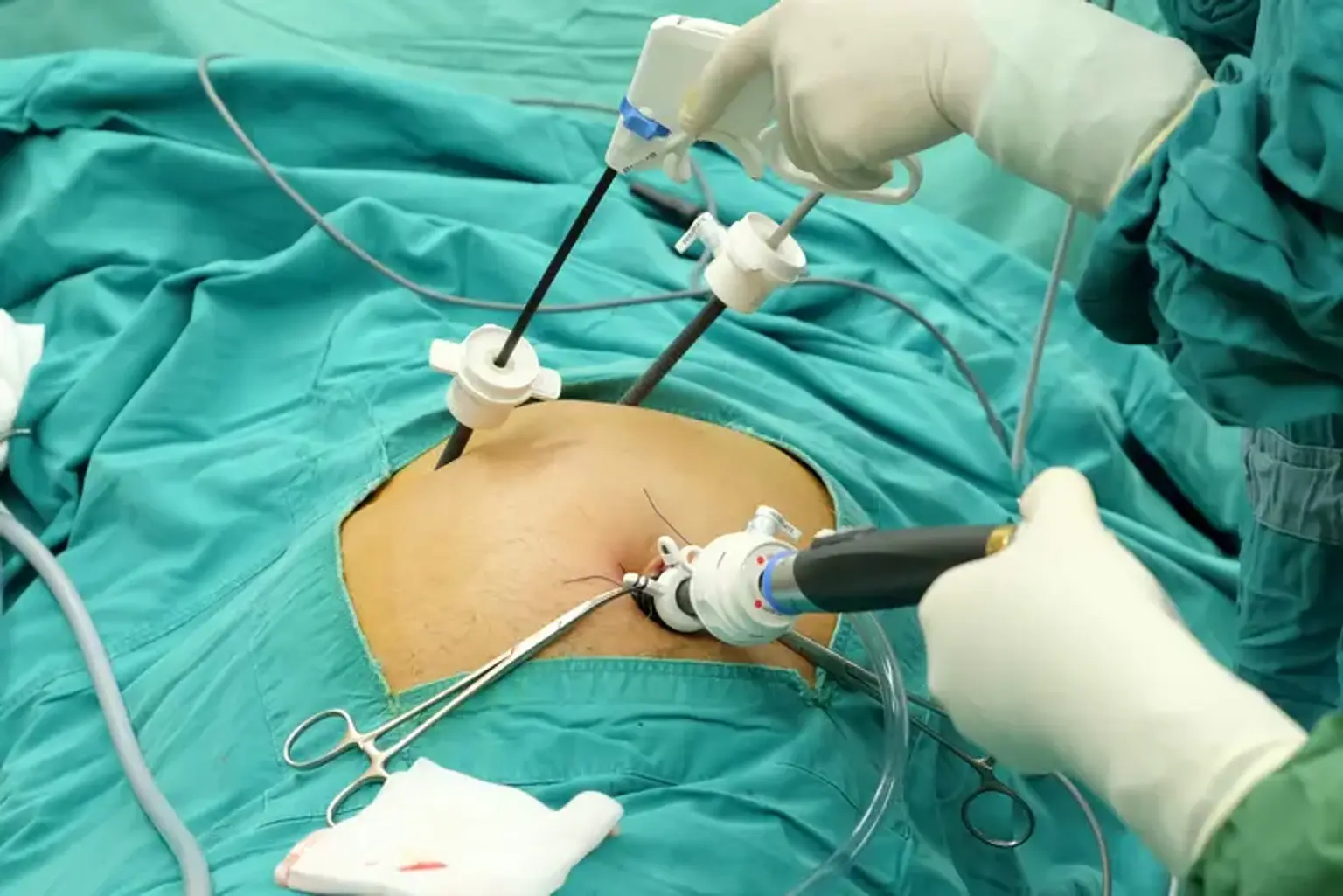
Laparoscopic cholecystectomy will commence after anaesthetic induction and intubation. It takes around an hour or two to do a laparoscopic cholecystectomy. A few tiny incisions will be made in your belly by a surgeon. Thin, hollow tubes will be inserted into the incisions by the surgeon. After that, the surgical team will insert a laparoscope and other surgical equipment into the tubes.
First, the abdomen is insufflated to 15 mmHg with carbon dioxide. Following that, four tiny incisions are made in the belly for trocar installation (supraumbilical x1, under the breastbone x1, and right subcostal x2). The gallbladder is retracted across the liver using a camera (laparoscope) and lengthy tools. This enables for the planned area of the hepato-cystic triangle to be exposed.
Careful dissection is used to get a critical view of safety. The elimination of fibrous and fatty tissue from the hepato-cystic triangle, the presence of just two tube structures entering the gallbladder's base, and the separation of the gallbladder's bottom third from the liver to disclose the cystic plate characterize this view.
After obtaining an adequate view of safety, the operating surgeon can proceed with assurance that the cystic duct and cystic artery have been separated. Both structures are carefully cut and transected. Using electrocautery or a harmonic scalpel, the gallbladder is then completely detached from the liver bed. After allowing the abdomen to deflate to 8 mmHg for 2 minutes, hemostasis should be established. This method is used to prevent missing possible venous bleeding caused by high intra-abdominal pressure (15 mmHg). The gallbladder is extracted from the abdomen in a specimen pouch. All trocars should be removed under direct vision. Closure of port sites is surgeon specific; closure of the fascia of trocar sites more than 5 mm to avoid incisional hernias in the postoperative phase.
What happens after laparoscopic cholecystectomy?
After surgery, your team will keep an eye on you for a few hours. They aim to ensure that you awaken from anesthesia without difficulties. They will examine your heart, respiration, blood pressure, and urination abilities (pee). If there are no complications, you should be able to go home the same day as your laparoscopic cholecystectomy. You may need to stay in the hospital for a day or two after having an open cholecystectomy.
To aid your recovery after surgery, do the following:
- Avoid lifting large objects.
- Drink lots of water.
- Consume fiber-rich meals to aid bowel movements (pooping).
- Follow your healthcare provider's recommendations for wound care and medication administration.
- Increase your activities gradually.
- Take a short walk every day to help avoid blood clots.
You should be able to drive and eat normally in a day or two if there are no issues. You should be able to return to work and other normal activities in approximately a week, as long as they don’t involve lifting. You may require a week or two before engaging in physical or sexual activity.
Without a gallbladder, you can live a completely normal existence. Your liver will continue to produce enough bile to digest your food, but instead of storing it in your gallbladder, it will drip continuously into your digestive system.
You may be instructed to follow a specific diet before to surgery, but this is not required following. Instead, strive for a generally healthy, balanced diet. Some patients develop bloating or diarrhea following surgery, although this normally resolves within a few weeks. If you notice that certain foods or drinks cause these symptoms, you should avoid them in the future.
Laparoscopic vs. open cholecystectomy
Several studies have found no significant differences in mortality, disease complications, or operational time between laparoscopic and open cholecystectomy. When compared to traditional open cholecystectomy, laparoscopic cholecystectomy has a much shorter hospital stay and faster recovery. These findings support the current preference for laparoscopic cholecystectomy over open cholecystectomy.
Your doctor or surgeon will advise you on whether an open or laparoscopic cholecystectomy is best for you. There are various advantages to the laparoscopic procedure:
- Less pain.
- Reduced chance of surgical complications.
- Faster recovery and return to normal activities.
- Less visible wounds and scars.
What are the possible complications associated with laparoscopic cholecystectomy?
Serious complications that occur with laparoscopic cholecystectomy, such as bile duct damage, bile leaks, hemorrhage, and intestinal injury, are caused in part by patient selection, surgical inexperience, and the technological limits inherent in the minimally invasive procedure.
These considerations, together with the inherent sequelae of biliary tract illnesses such as inflammation and scarring, have led to the notion of "Stop Rules" for surgeons doing this procedure. In essence, if a safe dissection cannot be achieved laparoscopically, an early conversion to an open method should be readily recognized as the appropriate course of action.
Serious complications occurred in 2.6 percent of 8856 laparoscopic cholecystectomies in a research that pooled data from seven big studies. A meta-analysis of eight large studies on laparoscopic cholecystectomies found the following types and frequencies of major complications: bleeding (0.11 to 1.97 percent), abscess (0.14 to 0.3 percent), bile leak (0.3 to 0.9 percent), biliary injury (0.26 to 0.6 percent), and bowel injury (0.14 to 0.35 percent). The laparoscopic technique has a lower risk of wound infections and surgical site infections than the open approach, but there is no advantage in terms of intra-abdominal abscess development.
Biliary injury:
Biliary injury may be detected during laparoscopic surgery; if so, conversion to an open procedure and treatment of the injury should be performed only if the surgeon is experienced in advanced biliary surgery. If so, the surgeon should seek intraoperative advice with a specialist who is knowledgeable with this issue.
External draining of the gallbladder fossa should be done before consulting a specialist. Biliary duct injuries should always be treated by a multidisciplinary team that includes a surgeon, diagnostic radiologist, interventional gastroenterologist, and interventional radiologist.
The majority of injuries are not noticed during the initial operation. Early bile duct damage following laparoscopic cholecystectomy is typically nonspecific, with patients complaining of vague abdominal discomfort, prolonged nausea and vomiting, and low-grade fever.
Bleeding complications:
Uncontrollable bleeding during laparoscopic cholecystectomy occurs at a rate of 0.1 to 1.9 percent and can originate from one of three locations: the liver, arterial sources, or port insertion sites. Significant bleeding from the liver bed is very frequent, and it is now recognized that it is caused by the often near proximity of the middle hepatic vein and its radicals to the gallbladder fossa in up to 10% to 15% of individuals. If early attempts at laparoscopic hemostatic control fail, bleeding commonly occurs during the last stages of gallbladder removal from the hepatic fossa and necessitates rapid conversion to open to control copious hemorrhage by stitch ligation.
Arterial control complications with the cystic artery can be diagnosed and managed quickly using clips. They may also appear postoperatively as an abrupt hemodynamic drop necessitating resuscitation, transfusions, and, in some cases, reoperation. In this case, the culprit is usually a dislodged clip.
Finally, incision or trocar site bleeding is possible. Patients frequently appear sub-acutely in the first few days after surgery. Direct view of trocar removal at the end of the laparoscopy is recommended so that, if necessary, such a problem may be treated with laparoscopically inserted sutures. When patients present with delayed bleeding, ultrasonography (US) testing might reveal a heterogeneous fluid accumulation, allowing the diagnosis of hematoma. If a US examination is inconclusive, abdominal wall and intraperitoneal hematomas might be seen as regions of increased attenuation on computed tomography (CT). If the patient is hemodynamically unstable, re-laparoscopy is recommended for direct examination.
Bowel injury:
Inadvertent intestinal damage has been reported in one to four instances out of 1000 laparoscopic surgeries in various studies. The clinical context dictates how this issue is managed. If the damage is discovered during surgery, an open procedure for repair is recommended if it cannot be fixed using the laparoscope.
Within 96 hours following the surgery, patients may experience trocar site discomfort, abdominal distention, diarrhea, leukopenia, and cardiovascular collapse due to sepsis. An emergency laparotomy is needed if the patient is sick or has free air in the abdomen. Standard enterocutaneous fistula maintenance with nutritional support, sufficient drainage, and wound care is effective in situations when the presentation is more indolent and controlled.
Post-cholecystectomy syndrome:
Postcholecystectomy syndrome (PCS) is a collection of symptoms that reoccur and remain following cholecystectomy, including prolonged stomach discomfort and dyspepsia.
PCS is classified as "early" if it starts immediately after surgery and "late" if it happens months or years afterwards. Pain and dyspepsia, often known as PCS, can be caused by a wide range of biliary and extra-biliary disorders. One-half of PCS patients are found to have biliary, pancreatic, or gastrointestinal diseases, with the remainder having extraintestinal illness.
PCS treatment is customized to the underlying cause of the symptoms. The underlying condition producing PCS is generally diagnosed utilizing imaging to search for retained or recurring stones or to find a bile duct leak, stricture, or transection. In most situations, ultrasonography and/or computed tomography (CT) scanning can be used, followed by direct cholangiography or magnetic resonance cholangiopancreatography (MRCP). For biliary tract examination, MRCP is a noninvasive alternative to direct cholangiography.
Conclusion
The gallbladder is a tiny organ located in the upper abdomen. The abdomen is a large region in the center of your body that houses several organs, including your stomach and gallbladder. The gallbladder collects and stores bile, a substance that aids digestion in the body. Gallstones are small, hard deposits that can develop in the gallbladder. This is a fairly common condition. If your gallstones create health difficulties, your doctor may recommend surgery to remove them. For example, if your gallbladder is no longer functioning properly and you are in pain, you may require surgery.
To remove the gallbladder, surgeons used to make a huge cut (incision) in the belly. This is known as open surgery. Today, surgeons can do this operation with a small equipment and a few tiny incisions. Laparoscopic surgery is so named because the main instrument is a laparoscope. Surgery with these small instruments is referred to as minimally invasive surgery.
Laparoscopic cholecystectomy reduces postoperative discomfort, reduces the requirement for postoperative analgesics, reduces the hospital stay from one week to less than 24 hours, and allows the patient to return to full activity within one week (compared with 1 month after open cholecystectomy). When compared to open cholecystectomy, laparoscopic cholecystectomy gives better cosmesis and patient satisfaction.
If the surgeon meets a problem that necessitates manual palpation and direct vision for repair, the laparoscopic treatment should be switched to an open procedure. If the necessity arises, surgeons should transition to open procedures without hesitation.