Overview
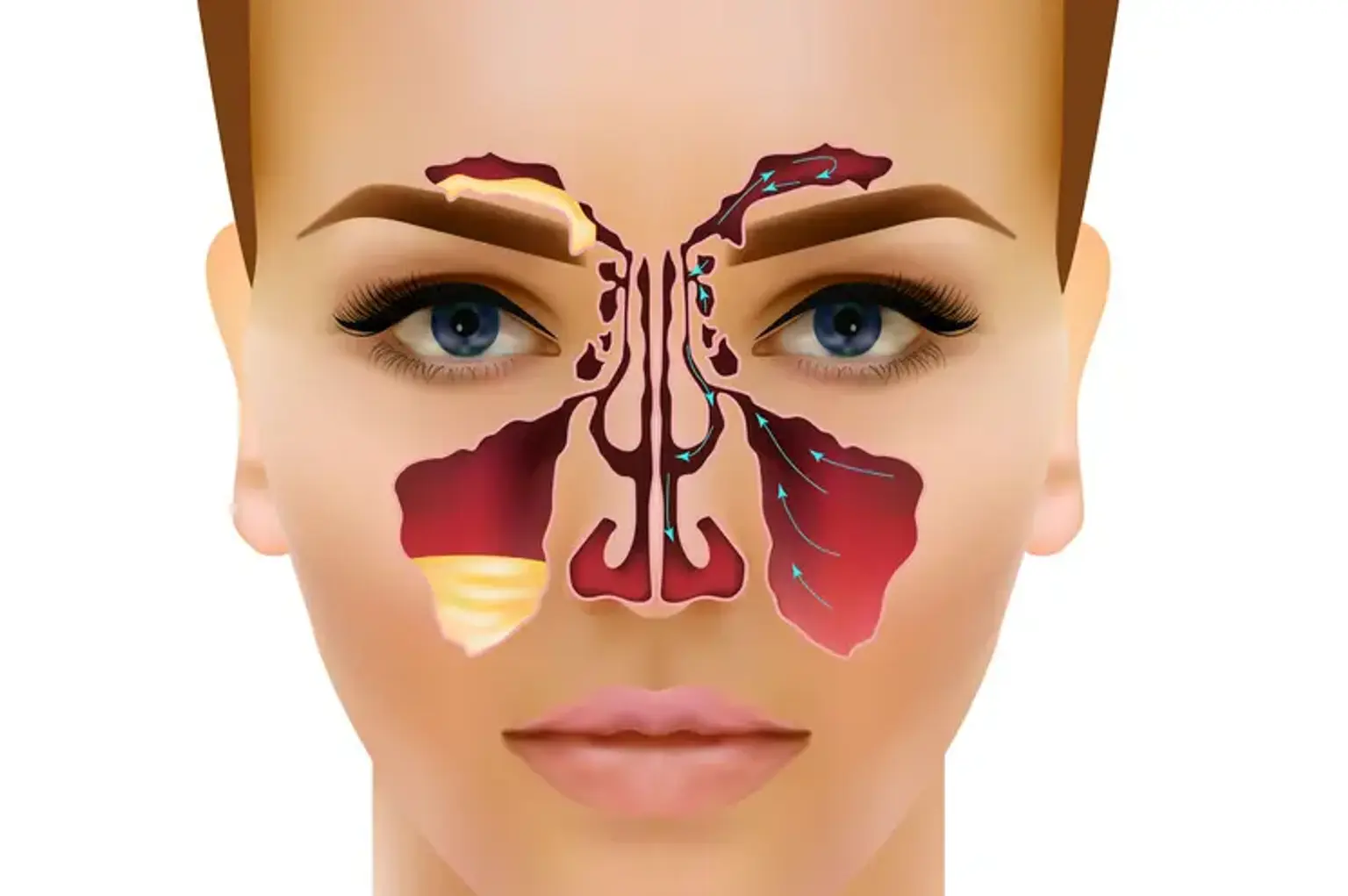
The maxillary sinuses are the largest of the paranasal sinuses, located behind the cheekbones on either side of the nose. They play a crucial role in the respiratory system, helping to filter and humidify the air we breathe. These sinuses also help reduce the weight of the skull and enhance the resonance of our voice. When the maxillary sinuses become blocked or inflamed, it can cause discomfort, pressure, and even facial deformities, making proper care and treatment essential for maintaining both health and appearance.
The importance of treating maxillary sinus issues goes beyond just alleviating pain. Conditions like infections, cysts, and volume loss can lead to chronic issues that affect a person's overall well-being and facial aesthetics. Treating these problems promptly can restore not only sinus health but also contribute to better quality of life and improved facial appearance.
What is Maxillary Sinus Treatment?
Maxillary sinus treatment refers to the procedures used to address a variety of issues that can affect the maxillary sinuses, such as infections, cysts, inflammation, and volume loss. These treatments can range from non-invasive options like medications and nasal sprays to more advanced procedures like surgery and volume restoration techniques.
One of the main goals of maxillary sinus treatment is to relieve symptoms such as pain, sinus pressure, and congestion. These symptoms often result from infections or inflammation that prevent the sinuses from draining properly. When these conditions become chronic, surgical intervention may be needed to correct blockages or restore lost sinus volume. Restoration of sinus volume is especially important for individuals experiencing facial sagging or asymmetry caused by the loss of soft tissue support around the sinuses.
In addition to medical benefits, many patients seek maxillary sinus treatment for cosmetic reasons. Treatments aimed at restoring the structure and volume of the sinuses can also improve facial appearance by lifting the cheek area and reducing the appearance of hollow or sunken cheeks.
Common Causes of Maxillary Sinus Issues
Several factors can contribute to problems with the maxillary sinuses. The most common causes include sinus infections (sinusitis), chronic inflammation, and cysts. Sinusitis occurs when the sinuses become inflamed, often due to an infection, which can cause swelling, mucus buildup, and pressure in the sinus cavities. Over time, this can lead to the formation of cysts or polyps that block sinus drainage.
Chronic sinusitis is particularly concerning because it lasts for months or even years, leading to persistent pain, pressure, and difficulty breathing through the nose. Chronic sinus conditions can also contribute to volume loss in the maxillary sinuses, affecting both the health of the sinuses and the appearance of the face. Aging is another significant factor in maxillary sinus issues, as the natural volume in the face decreases over time, which can exacerbate sinus-related problems.
In addition to these factors, environmental influences such as allergens, pollutants, or sinus trauma from accidents or surgery can increase the likelihood of maxillary sinus problems.
Symptoms and Diagnosis of Maxillary Sinus Problems
Maxillary sinus issues often present with clear symptoms, which can include facial pain or pressure, nasal congestion, headache, and a feeling of fullness around the cheekbones. Other signs may include post-nasal drip, a reduced sense of smell, and fatigue. If left untreated, these symptoms can worsen, leading to more severe discomfort and complications.
To diagnose maxillary sinus problems, doctors may use several diagnostic tools. A physical exam may reveal tenderness around the cheekbones or nose, while imaging techniques such as CT scans provide detailed views of the sinus cavities to identify blockages, infections, or structural issues. Endoscopic sinus exams, where a small camera is inserted into the nasal passages, can also help identify the exact cause of sinus problems and guide treatment decisions.
Diagnosing maxillary sinus issues early is important for preventing long-term damage. For example, if a sinus infection is left untreated, it can lead to the development of cysts or chronic inflammation that could require more extensive treatment, including surgery. Identifying the cause of sinus issues ensures that patients receive the most appropriate treatment, whether it's a simple medication regimen or a more complex surgical procedure.
Sinus Infection Treatment Options
When it comes to treating sinus infections, there are a variety of options available, depending on the severity and duration of the condition. For acute sinus infections, which are often caused by viruses, the primary treatment is typically conservative, such as rest, hydration, and over-the-counter medications. Decongestants and saline nasal sprays can help relieve symptoms by reducing nasal congestion and promoting sinus drainage.
In cases of bacterial infections, antibiotics may be prescribed to target the underlying infection. However, antibiotics are not effective for viral infections, and overuse can lead to antibiotic resistance. For chronic sinus infections, which last for 12 weeks or more, treatment may include long-term medication, corticosteroid nasal sprays, or even allergy medications if allergies are a contributing factor. Chronic sinusitis may also require surgery if the sinuses are not responding to other treatments, such as endoscopic sinus surgery.
The goal of sinus infection treatments is to reduce inflammation, clear blocked sinuses, and restore proper sinus function. By addressing the root cause of the infection, treatments can help improve overall sinus health and prevent future infections.
Sinus Surgery: When is it Required?
Sinus surgery becomes necessary when other treatment options, such as medications and nasal therapies, fail to resolve the symptoms or if the sinus issues are causing significant discomfort or complications. The primary goal of sinus surgery is to improve sinus drainage, remove blockages, and reduce inflammation to restore normal sinus function. Surgical procedures are typically considered when:
Chronic sinusitis persists despite medical treatment.
Sinus infections recur frequently or last for extended periods.
There are structural abnormalities, such as a deviated septum or nasal polyps, that prevent proper drainage.
Cysts or tumors are obstructing the sinuses and causing symptoms.
The two main types of sinus surgery are functional endoscopic sinus surgery (FESS) and maxillary sinus surgery. FESS is the most common method for treating chronic sinusitis and involves the removal of inflamed tissue, polyps, or other obstructions using an endoscope. Maxillary sinus surgery may be required if there is significant damage or volume loss in the maxillary sinuses.
While sinus surgery is effective in providing long-term relief for many patients, it carries certain risks, including infection, bleeding, or damage to surrounding structures. A qualified and experienced surgeon will assess the severity of the sinus issue and recommend the most appropriate surgical approach.
Endoscopic Sinus Surgery
Endoscopic sinus surgery (ESS) is a minimally invasive procedure used to treat chronic sinus conditions, such as sinusitis, nasal polyps, or structural issues that affect sinus drainage. The procedure involves inserting a thin, flexible tube with a light and camera (endoscope) through the nostrils to examine the sinuses and identify any obstructions or damaged tissue. Surgical instruments are then used through the endoscope to remove blockages, correct deformities, or clear up inflamed tissue.
One of the key benefits of endoscopic sinus surgery is that it does not require external incisions, leading to a quicker recovery and less post-operative pain compared to traditional sinus surgery. The procedure can be performed on an outpatient basis under general anesthesia, and patients can often return to their normal activities within a few days, although full recovery can take several weeks.
Endoscopic sinus surgery is highly effective for treating chronic sinusitis and improving overall sinus function. However, like any surgery, it carries some risks, including bleeding, infection, and injury to surrounding structures such as the eyes or teeth. It’s important for patients to follow post-surgical care instructions to minimize complications and promote optimal healing.
For many patients, endoscopic sinus surgery offers a significant improvement in their quality of life, alleviating chronic symptoms and preventing future sinus infections.
Chronic Sinusitis Treatment
Chronic sinusitis, characterized by persistent inflammation of the sinuses, can be difficult to treat and may require a combination of medical and surgical interventions. This condition often results in prolonged nasal congestion, facial pain, and sinus pressure that can interfere with daily life. While acute sinus infections can be treated with antibiotics, chronic sinusitis often requires more comprehensive care.
Initial treatment for chronic sinusitis may involve a course of corticosteroids to reduce inflammation, nasal saline irrigation to help clear mucus, and possibly oral antibiotics if an infection is present. For patients whose symptoms are not relieved by these treatments, surgery may be necessary to open up blocked sinus passages and improve drainage. The most common surgical procedure for chronic sinusitis is endoscopic sinus surgery (ESS), which uses a small camera and instruments inserted through the nose to remove blockages or damaged tissue without the need for large incisions.
Endoscopic sinus surgery offers a minimally invasive approach with a shorter recovery time compared to traditional surgery. However, it is important to note that surgery may not completely cure chronic sinusitis. Ongoing maintenance treatments, such as nasal sprays and lifestyle changes, are often required to manage the condition long-term.
Sinus Volume Restoration Procedures
Sinus volume loss occurs when the soft tissue and bone structure around the sinuses deteriorate, leading to facial sagging or sunken cheeks. This can happen naturally with age, following sinus surgery, or due to chronic sinus conditions. Restoring the volume in the maxillary sinuses is important not only for improving sinus health but also for enhancing facial aesthetics.
One of the most common approaches to restoring sinus volume is fat grafting. This procedure involves harvesting fat from another area of the patient’s body (usually the abdomen or thighs) and injecting it into the affected area of the face or sinuses. Fat grafting can help restore the natural contours of the face, improving both facial volume and sinus function.
In some cases, injectable dermal fillers containing hyaluronic acid may be used as a temporary solution for volume restoration. These treatments are less invasive and can offer immediate results, though they may require maintenance treatments to maintain the desired effect.
Sinus volume restoration plays an important role in both improving sinus function and addressing aesthetic concerns, particularly for those with aging-related facial changes.
Maxillary Sinus Cyst Treatment
Maxillary sinus cysts are fluid-filled sacs that form in the sinus cavities. These cysts are generally benign but can cause discomfort, pain, and blockages in the sinuses. Symptoms may include facial swelling, pressure, nasal congestion, and sometimes headaches.
Treatment for maxillary sinus cysts depends on the size and severity of the cyst. If the cyst is small and not causing significant symptoms, it may not require treatment other than monitoring. However, larger cysts or those that cause chronic sinus infections may require surgical intervention.
The most common procedure to remove a sinus cyst is endoscopic sinus surgery, which allows surgeons to remove the cyst through the nasal passages with minimal disruption to surrounding tissues. In more severe cases, a procedure called maxillary sinusotomy may be performed to drain the cyst and prevent future blockages.
For patients with recurring cysts, sinus volume restoration techniques may be used in combination to ensure proper sinus function and reduce the risk of further complications.
Non-Surgical Maxillary Sinus Treatment for Volume Loss
Non-surgical treatments for maxillary sinus volume loss focus on restoring facial volume and improving sinus health without the need for invasive procedures. These treatments are ideal for patients who want to avoid surgery or are looking for a less invasive solution.
Injectable dermal fillers are the most popular non-surgical option for restoring volume in the maxillary sinus area. Hyaluronic acid-based fillers, like Juvederm and Restylane, can be injected into the areas around the sinuses to lift and plump the cheeks, offering immediate results with minimal downtime. These treatments can help reduce the appearance of sagging and hollow cheeks, which often result from sinus volume loss.
Another non-invasive option is PRP (Platelet-Rich Plasma) therapy, which uses the patient's own blood to promote healing and tissue regeneration. While PRP is more commonly used in facial rejuvenation, it may be an option for patients seeking to improve the health and volume of their maxillary sinuses.
Although these non-surgical treatments offer temporary results, they can be an effective solution for individuals who want to address sinus volume loss without the risks or downtime associated with surgery.
Sinus Pressure Relief Treatments
Sinus pressure is a common symptom of sinus infections and other sinus-related conditions. The buildup of mucus or inflammation in the sinus cavities can lead to a feeling of heaviness or pain in the face, particularly around the cheeks, eyes, and forehead.
Sinus pressure relief treatments aim to reduce this discomfort by improving sinus drainage and reducing inflammation. The most common methods include:
Saline nasal irrigation: Using a saline solution to rinse the nasal passages helps flush out mucus, allergens, and irritants, providing immediate relief from pressure.
Decongestants: Oral or nasal decongestants can reduce swelling in the nasal passages, improving airflow and helping the sinuses drain more effectively.
Warm compresses: Applying a warm compress to the face can help open up the sinus passages and alleviate pain.
Steam inhalation: Breathing in steam from a hot shower or a bowl of hot water can help loosen mucus and relieve sinus pressure.
For more persistent cases of sinus pressure, especially those caused by chronic sinusitis or structural issues, surgical interventions, such as endoscopic sinus surgery, may be required to address the underlying problem. In these cases, surgical treatments can provide long-term relief by removing blockages and improving sinus drainage.
Recovery After Maxillary Sinus Surgery
After undergoing maxillary sinus surgery, patients can expect a recovery period that typically lasts a few days to a couple of weeks, depending on the complexity of the procedure. For minimally invasive surgeries like endoscopic sinus surgery, recovery is usually quicker compared to traditional sinus surgery.
Immediately following surgery, patients may experience mild discomfort, nasal congestion, and slight bleeding. Pain management often involves over-the-counter medications or prescribed pain relievers. Swelling around the eyes and nose is common but typically subsides within a few days.
During the recovery period, it’s important to follow post-operative instructions, such as avoiding strenuous activities, refraining from blowing the nose, and using saline sprays to keep the sinuses clear. Most patients can return to normal activities within 7-10 days, but full healing may take up to 4 weeks. Regular follow-up visits with the surgeon are essential to monitor healing and ensure the sinuses are functioning properly.
Sinus Treatment Recovery: Dos and Don’ts
To ensure optimal recovery after sinus treatment or surgery, patients must adhere to specific guidelines. Dos include:
Follow-up care: Regular visits to the doctor to monitor healing and ensure there are no complications.
Hydrate well: Staying hydrated helps keep the mucus thin and promotes drainage.
Use prescribed medications: Follow the doctor’s instructions for antibiotics, nasal sprays, and pain medications.
Don’ts include:
Avoid vigorous physical activity: Strenuous exercise can increase swelling and hinder healing.
Don’t blow your nose forcefully: This can disrupt the healing process and lead to bleeding or infections.
Avoid irritants: Stay away from smoke, dust, and strong chemicals that can aggravate the sinuses.
Proper adherence to these dos and don’ts will promote faster healing and reduce the risk of complications.
Maxillary Sinus Treatment and Surgery in Korea
Korea has become a global leader in the field of medical and cosmetic procedures, including maxillary sinus treatments and surgeries. Known for its advanced technology, skilled practitioners, and state-of-the-art facilities, Korea offers high-quality care for both sinus health and aesthetic procedures.
Many international patients travel to Korea for sinus treatments due to its reputation for exceptional care and innovative approaches, particularly in endoscopic sinus surgery and sinus volume restoration. Surgeons in Korea are highly trained and often specialize in minimally invasive techniques, which help reduce recovery times and improve patient outcomes.
Additionally, Korea's medical tourism industry is well-established, with many hospitals offering packages that include treatment, accommodation, and travel assistance for international patients. For those seeking both functional and aesthetic improvements, Korea offers a unique opportunity for comprehensive care.
Maxillary Sinus Volume Restoration in Korea: Leading Procedures
Maxillary sinus volume restoration is gaining popularity in Korea, where advanced techniques such as fat grafting and hyaluronic acid fillers are used to not only restore sinus health but also enhance facial aesthetics. Many patients seeking treatment for sinus volume loss are also looking to improve their facial appearance, making Korea an ideal destination for those who want both medical and cosmetic benefits.
Fat grafting, a popular procedure in Korea, involves harvesting fat from one area of the body and injecting it into the maxillary sinus region to restore volume. This procedure can help correct the effects of aging or sinus-related volume loss, creating a more youthful, fuller facial appearance.
Korean clinics also offer hyaluronic acid-based injectable fillers to address non-surgical volume loss in the sinuses. These treatments provide immediate results with minimal downtime and are often chosen by patients who prefer a less invasive approach.
Korea's expertise in combining sinus treatment with cosmetic restoration ensures that patients receive comprehensive care, improving both their sinus health and facial aesthetics.
Costs and Considerations for International Patients Seeking Sinus Treatment in Korea
For international patients seeking maxillary sinus treatments in Korea, the cost can vary based on the procedure and the clinic. Generally, Korea offers more affordable options compared to Western countries, making it an attractive destination for medical tourism. Procedures like endoscopic sinus surgery or sinus volume restoration tend to be more affordable in Korea, with prices often ranging from $2,000 to $4,000 USD.
In addition to the cost of the procedure, patients should factor in the costs of travel, accommodation, and post-operative care. Many Korean hospitals offer all-inclusive packages that include treatment, stay, and transport, making it easier for international patients to manage logistics.
While cost is an important consideration, the quality of care should always come first. Opting for reputable hospitals and qualified surgeons is essential to ensure the best possible results and a smooth recovery.
Benefits of Maxillary Sinus Treatment
Maxillary sinus treatment offers numerous benefits for both health and aesthetics. By addressing sinus issues, such as infections, cysts, and volume loss, patients can experience significant relief from chronic symptoms like facial pressure, nasal congestion, and headaches.
For patients with sinus volume loss, restoration procedures not only improve sinus function but also enhance facial aesthetics. Restoring lost volume can lift sagging cheeks, reduce the appearance of hollow areas, and create a more youthful, natural facial contour.
Beyond cosmetic improvements, proper sinus treatment can also reduce the risk of future sinus infections and improve overall sinus health, leading to a better quality of life.
Potential Risks of Maxillary Sinus Surgery
Like any surgical procedure, maxillary sinus surgery carries potential risks. These include infection, bleeding, and scarring. In some cases, complications may arise if the sinuses do not fully heal or if there is damage to surrounding structures, such as the eyes or teeth.
However, the risks can be minimized by selecting an experienced surgeon and following all pre- and post-operative care instructions. Endoscopic sinus surgery, which is minimally invasive, generally offers lower risks and quicker recovery times compared to traditional surgery.
While the risks are real, many patients find that the benefits of improved sinus health and facial appearance outweigh them, making surgery a worthwhile option for those who require more advanced treatments.
Frequently Asked Questions (FAQs)
How long does recovery take after sinus surgery?
Recovery typically takes about 7-10 days for minimal pain and swelling, with full healing potentially taking 3-4 weeks.
Can non-surgical treatments restore sinus volume?
Yes, non-surgical treatments like injectable dermal fillers can restore volume, though results are temporary and may require maintenance.
Is maxillary sinus surgery safe?
Yes, when performed by an experienced surgeon, maxillary sinus surgery is generally safe. Endoscopic methods, in particular, minimize risks.
Why is Korea a popular destination for sinus treatments?
Korea is known for its advanced technology, skilled surgeons, and affordability, making it a top destination for sinus treatments and cosmetic surgeries.
How effective is fat grafting for sinus volume restoration?
Fat grafting is highly effective for restoring sinus volume and enhancing facial contours, with long-lasting results in many cases.
Patients can have peace of mind knowing that with proper care, maxillary sinus treatment can be a successful, life-changing procedure.
Conclusion
Maxillary sinus treatment plays a crucial role in both restoring sinus health and improving facial aesthetics. Whether addressing chronic sinus infections, volume loss, or structural issues, the right treatment can significantly enhance a patient's quality of life. From non-surgical options like injectable fillers to advanced procedures like endoscopic sinus surgery and fat grafting, there are a variety of approaches to meet individual needs.
For those considering treatment abroad, Korea stands out as a leading destination for maxillary sinus procedures, offering cutting-edge medical care, affordable pricing, and a combination of health and cosmetic benefits. With skilled practitioners and a focus on minimally invasive techniques, patients can expect excellent results and a smoother recovery.
Ultimately, whether seeking relief from sinus pressure, restoring lost volume, or enhancing facial appearance, maxillary sinus treatment can offer life-changing improvements. It's important to consult with qualified healthcare professionals to choose the best treatment plan, ensuring both health and beauty are restored with minimal risk.