Introduction
Metabolic Bone Disorders (MBD) refer to a group of conditions that affect bone strength and structure. These disorders occur when there are abnormalities in the metabolism of bone minerals like calcium, vitamin D, or phosphorus, leading to weakened bones.
The most common forms include osteoporosis, osteomalacia, and Paget's disease. These conditions can increase the risk of fractures, deformities, and serious disabilities. Early diagnosis and treatment are crucial for preventing further bone damage and improving quality of life.
Understanding the Causes of Metabolic Bone Disorders
Metabolic Bone Disorders have various causes, often linked to imbalances in essential minerals or hormones that regulate bone health.
Genetics: Some MBDs are hereditary, passed down through families.
Mineral Deficiencies: Low levels of calcium, phosphorus, or vitamin D disrupt bone formation.
Hormonal Imbalances: Disorders like hyperparathyroidism and low estrogen levels can lead to weakened bones.
Kidney Disease: Chronic kidney problems can affect calcium and phosphorus metabolism, increasing the risk of bone disease.
Medications: Long-term use of certain drugs, such as steroids or anticonvulsants, can also contribute to MBD.
Each of these factors can disrupt the normal bone-building process, making bones fragile and more susceptible to fractures.
Symptoms of Metabolic Bone Disorders
The symptoms of metabolic bone disorders vary based on the condition, but some common signs include:
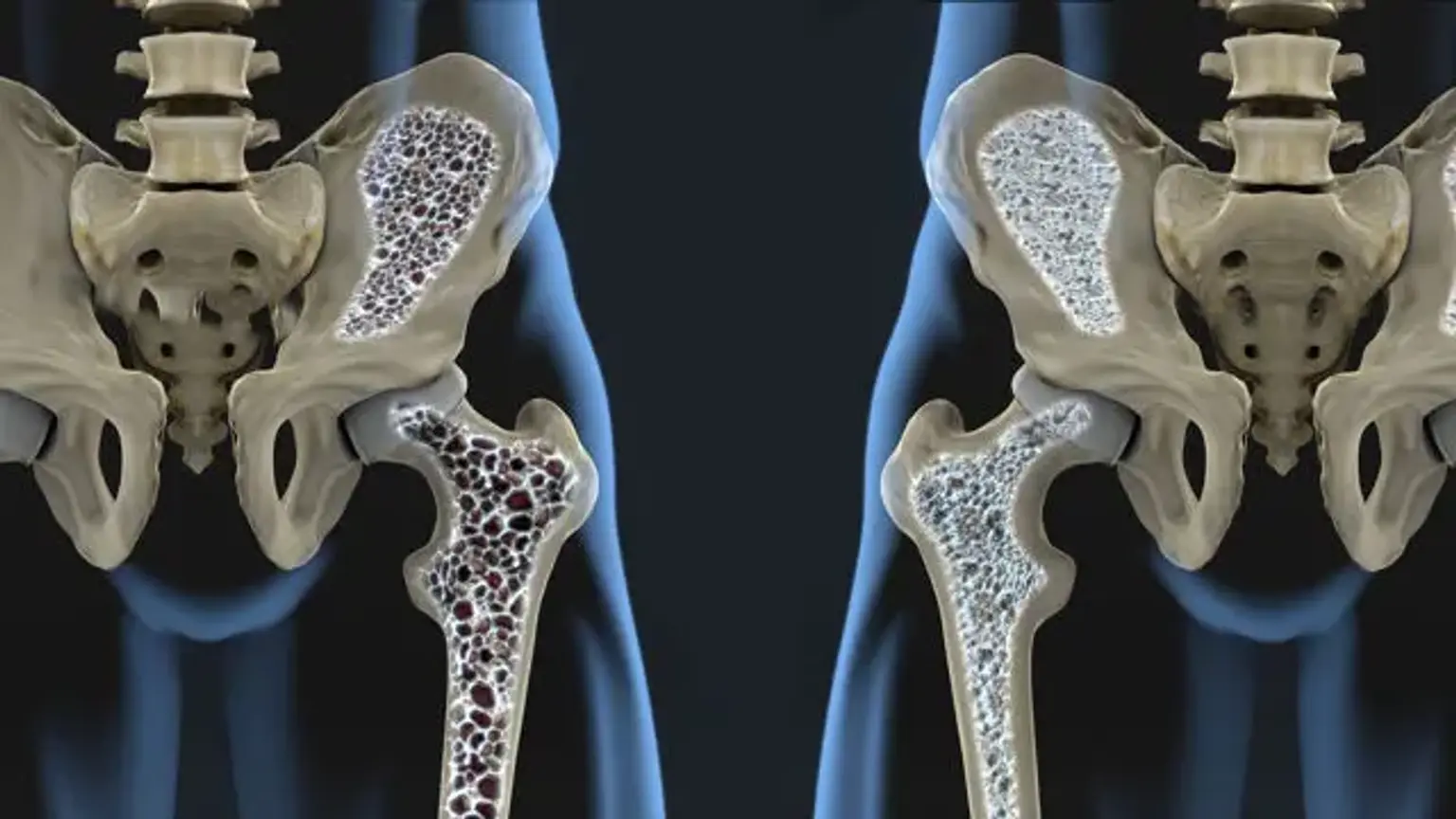
Osteoporosis: Often referred to as a “silent disease,” osteoporosis usually presents no symptoms until a fracture occurs. Symptoms may include back pain, loss of height, or a stooped posture due to vertebral fractures.
Osteomalacia: Bone pain, muscle weakness, and frequent fractures are typical signs. The pain often worsens at night and may affect the hips, pelvis, or legs.
Paget’s Disease: This condition can cause bone deformities, joint pain, and fractures. In some cases, the affected bones become enlarged or misshapen, leading to visible deformities.
In many cases, these symptoms develop slowly and may not be immediately noticeable, which is why regular screening is important for early detection.
Risk Factors for Developing Metabolic Bone Disorders
Several factors increase the likelihood of developing metabolic bone disorders:
Age: Older adults, particularly women after menopause, are at higher risk due to decreased estrogen levels, which help protect bone density.
Gender: Women are more likely to develop osteoporosis, especially post-menopausal women who experience a significant drop in estrogen.
Family History: Genetics play a crucial role; a family history of osteoporosis or other metabolic bone conditions can increase the risk.
Lifestyle Factors: Smoking, excessive alcohol consumption, and lack of physical activity can weaken bones over time.
Medical Conditions: People with conditions like chronic kidney disease, hyperthyroidism, or eating disorders may have a higher risk of developing MBD.
Medications: Long-term use of steroids, anticonvulsants, or certain cancer treatments can lead to bone loss.
Understanding these risk factors is vital for taking proactive steps toward prevention and early intervention.
Medications for Metabolic Bone Disorders
Several medications are available to help manage metabolic bone disorders, each with different mechanisms and benefits. Here’s an overview of the most commonly prescribed options:
Bisphosphonates: These are the cornerstone of osteoporosis treatment. They include oral options like alendronate and ibandronate, as well as intravenous forms like zoledronic acid. Bisphosphonates work by inhibiting the activity of osteoclasts (cells that break down bone tissue), thus slowing bone loss and improving bone density.
Anabolic Agents: Teriparatide (Forteo) is a synthetic form of parathyroid hormone, which stimulates new bone formation. This is generally prescribed for patients with severe osteoporosis who are at high risk of fractures.
Denosumab: This biologic therapy is given via injection and works by inhibiting the activity of osteoclasts. It’s used for people who have not responded to bisphosphonates or cannot tolerate them.
Hormone Replacement Therapy (HRT): In postmenopausal women, HRT can help replace estrogen, which is vital for maintaining bone density. However, its use is generally limited to individuals who are also experiencing menopausal symptoms.
Calcitonin: This hormone treatment helps regulate calcium levels in the body and can reduce pain associated with vertebral fractures, though it’s not commonly used as a first-line treatment.
These medications are typically prescribed based on the specific metabolic bone disorder, the patient’s overall health, and their response to previous treatments.
How Metabolic Bone Disorders Are Diagnosed
Diagnosing metabolic bone disorders involves a combination of medical history, physical exams, and various tests to assess bone health. Here’s how doctors typically approach the diagnosis:
Physical Examination: The doctor will check for physical signs such as fractures, deformities, or pain in bones and joints.
Bone Density Test (DEXA Scan): This test measures bone mineral density (BMD) and helps diagnose osteoporosis. Low BMD indicates weaker bones, increasing fracture risk.
X-rays: Useful for detecting fractures, deformities, or changes in bone structure. X-rays can also identify conditions like Paget's disease.
Blood Tests: These help assess calcium, vitamin D, phosphorus, and other minerals in the body. Low levels may indicate mineral imbalances affecting bone health.
Bone Scans: An isotope bone scan can identify areas of bone weakness or deformities, distinguishing between fractures caused by osteoporosis or malignancy.
These tests help doctors determine the underlying cause of the bone issues, allowing for a tailored treatment plan.
The Role of Surgery in Severe Cases
While most cases of metabolic bone disorders can be managed with medications and lifestyle changes, surgery may be necessary in more severe instances. Surgery is typically reserved for cases with significant bone deformities, fractures, or joint damage. Common surgical interventions include:
Spinal Fusions: In cases of osteoporosis or Paget’s disease that lead to spinal fractures or deformities, a spinal fusion may be performed to stabilize the spine and alleviate pain.
Hip Replacement: Severe fractures, especially those caused by osteoporosis, may require a hip replacement to restore mobility and prevent further complications.
Joint Replacement: Paget’s disease often leads to deformities in the joints, causing pain and limited movement. In such cases, joint replacement surgery may be needed.
Fracture Repair: If a patient experiences a bone fracture that does not heal properly, surgical intervention may be required to realign the bone or use hardware (e.g., screws, plates) to stabilize it.
Surgery can help restore function, alleviate pain, and improve the quality of life for those suffering from severe bone damage. However, it’s typically considered after other treatments have been tried.
Advances in Metabolic Bone Disorder Treatments
Recent advancements have significantly improved the treatment of metabolic bone disorders, focusing on more effective and personalized therapies.
Biologics: Medications like denosumab (Prolia) target specific pathways in bone metabolism, offering an alternative for patients who don’t respond to traditional drugs.
Gene Therapy: Although still experimental, gene therapies aim to correct genetic causes of conditions like Paget's disease, potentially offering long-term solutions.
Targeted Drugs: New drugs, such as romosozumab, help stimulate bone formation while inhibiting bone resorption, showing promising results for osteoporosis.
Technology: Digital tools and monitoring systems allow better tracking of bone health, aiding in real-time adjustments to treatment plans.
These advances offer hope for better outcomes and more individualized care for patients with metabolic bone disorders.
Non-Surgical Treatment Options
Treatment for metabolic bone disorders focuses on restoring bone health and preventing fractures. Non-surgical options are the first line of treatment and often include the following:
Calcium and Vitamin D Supplements: These are essential for bone health. Vitamin D helps the body absorb calcium, which is crucial for maintaining bone strength. Depending on the condition, doctors may prescribe different dosages.
Bisphosphonates: Medications like alendronate and risedronate help slow bone loss and improve bone density. They’re commonly prescribed for osteoporosis and osteomalacia.
Anabolic Agents: Teriparatide is a hormone therapy that stimulates bone growth and is used for severe osteoporosis. It’s typically prescribed when other treatments don’t provide adequate results.
Denosumab (Prolia): This injectable medication helps prevent bone breakdown by inhibiting osteoclast activity. It's an option for people who cannot take bisphosphonates.
Physical Therapy: Aimed at strengthening muscles and improving balance, physical therapy reduces the risk of falls and fractures. It may also include exercises designed to improve bone density.
These treatments can significantly improve bone strength, reduce fracture risk, and alleviate symptoms of pain or weakness.
Managing Pain and Discomfort
Pain management is a critical aspect of treating metabolic bone disorders, as they often cause chronic discomfort and reduce quality of life.
Medications: Nonsteroidal anti-inflammatory drugs (NSAIDs) and opioids may be prescribed for pain relief. Calcitonin can also be used for pain relief in vertebral fractures.
Physical Therapy: Targeted exercises strengthen muscles, improve flexibility, and reduce the risk of falls, which can alleviate pain from joint stress and bone weakness.
Non-invasive Treatments: Acupuncture, massage therapy, and chiropractic care may also provide relief for some patients.
Psychological Support: Chronic pain can lead to emotional strain. Support groups, counseling, and cognitive therapy can help patients cope with pain’s psychological effects.
These approaches combine to provide comprehensive relief, improving both physical and emotional well-being.
Preventive Measures for Metabolic Bone Disorders
Prevention is key in managing metabolic bone disorders. Early intervention can reduce the risk of severe fractures and improve long-term health outcomes.
Regular Screenings: DEXA scans and blood tests help detect bone density loss early, allowing for timely treatment.
Diet and Nutrition: A diet rich in calcium, vitamin D, and phosphorus is essential for bone health. Foods like dairy, leafy greens, and fortified cereals should be part of a daily diet.
Exercise: Weight-bearing activities like walking, running, and resistance training are crucial for building and maintaining strong bones.
Lifestyle Changes: Avoid smoking and excessive alcohol consumption, both of which contribute to bone loss.
Bone Health Education: Educating patients, especially those at higher risk (e.g., postmenopausal women), on the importance of diet, exercise, and medication adherence can reduce the incidence of MBD.
Preventive measures can greatly reduce the likelihood of developing serious bone-related issues, especially for those at risk.
Diet and Nutrition for Bone Health
A balanced diet plays a crucial role in preventing and managing metabolic bone disorders. Proper nutrition supports bone strength and function.
Calcium: Essential for bone structure, calcium-rich foods like dairy products, leafy greens, and tofu should be prioritized. Adults need about 1,000–1,200 mg of calcium daily.
Vitamin D: This vitamin enhances calcium absorption and supports bone remodeling. Sunlight, fortified foods (like milk and cereals), and fatty fish (like salmon) are great sources of vitamin D.
Phosphorus: Found in foods like meat, fish, and nuts, phosphorus is necessary for bone health, working alongside calcium and vitamin D.
Magnesium: This mineral helps with bone formation and muscle function. Nuts, seeds, and whole grains are good sources.
Avoid Deficiencies: Lack of key nutrients like calcium or vitamin D can weaken bones and increase the risk of fractures. Supplements are often recommended for individuals who struggle to meet dietary needs.
Maintaining a balanced diet with adequate nutrients is crucial for supporting bone density and overall skeletal health.
Lifestyle Changes to Support Bone Health
Adopting healthy lifestyle habits is essential in managing metabolic bone disorders and improving overall bone health.
Exercise: Regular weight-bearing exercises like walking, hiking, and weightlifting help stimulate bone formation and prevent further bone loss.
Quit Smoking: Smoking reduces bone density and impairs the body’s ability to absorb calcium, increasing fracture risk.
Limit Alcohol: Excessive alcohol intake can interfere with calcium absorption and lead to weaker bones over time.
Fall Prevention: Installing grab bars, using non-slip mats, and ensuring good lighting can prevent falls, which are especially dangerous for individuals with weakened bones.
Incorporating these changes can significantly reduce the risk of fractures and improve bone health over time.
Psychological Impact of Metabolic Bone Disorders
The emotional toll of living with a metabolic bone disorder can be significant. Chronic pain, limited mobility, and concerns about future fractures can lead to feelings of anxiety, depression, and isolation.
Coping Strategies: Therapy, mindfulness, and stress management techniques can help patients deal with the mental and emotional challenges.
Support Groups: Connecting with others facing similar challenges can offer emotional support and practical advice.
Quality of Life: Proper treatment, pain management, and lifestyle modifications can improve both physical and emotional well-being, allowing individuals to lead fulfilling lives.
Addressing mental health alongside physical care is critical for the overall well-being of patients.
Global Prevalence of Metabolic Bone Disorders
Metabolic bone disorders affect millions of people worldwide, with some regions experiencing higher rates due to genetic, environmental, and lifestyle factors.
Osteoporosis: It is most common in postmenopausal women, but it can also affect men, especially in later life. In the U.S. alone, an estimated 10 million people have osteoporosis.
Paget’s Disease: This condition affects 1–2% of people over 50 in some countries, particularly in Europe and North America.
Geographic Variations: In countries with lower sunlight exposure, like northern Europe, vitamin D deficiency is more common, leading to higher rates of osteomalacia and rickets.
Understanding these global patterns can help tailor prevention strategies and public health initiatives.
Cost and Accessibility of Treatment
The cost of treating metabolic bone disorders can be a significant concern for many patients, particularly in areas with limited healthcare access.
Medication Costs: Treatments like bisphosphonates, denosumab, and anabolic agents can be expensive, especially when used long-term.
Insurance Coverage: In some regions, insurance plans may not fully cover the costs of osteoporosis medications or bone density tests, creating barriers for patients who need care.
Access to Specialists: Access to endocrinologists, rheumatologists, or orthopedic specialists may be limited in rural or underserved areas, making it harder for patients to receive proper diagnosis and treatment.
Governments and healthcare systems need to address these disparities to ensure that all patients have access to affordable care and medications.
Prognosis and Long-Term Outlook
The prognosis for individuals with metabolic bone disorders depends on several factors, including the severity of the condition, age, treatment response, and adherence to lifestyle changes.
Osteoporosis: With early diagnosis and proper treatment, people with osteoporosis can manage the condition effectively, reducing the risk of fractures and maintaining mobility.
Paget’s Disease: While Paget’s disease is a chronic condition, appropriate treatment can help manage symptoms and prevent complications like deformities and fractures.
Osteomalacia: With proper vitamin D and calcium supplementation, most people with osteomalacia can recover fully, especially if treated early.
Chronic Management: Metabolic bone disorders often require lifelong management, but with ongoing treatment and regular monitoring, patients can live active, pain-free lives.
The key to a favorable long-term outlook lies in early intervention, consistent treatment, and lifestyle adjustments.
Role of Family and Caregivers
Family members and caregivers play an essential role in supporting individuals with metabolic bone disorders, especially when the condition leads to disability or chronic pain.
Encouraging Treatment Adherence: Helping patients stick to their medication schedules and regular physical therapy can improve outcomes.
Emotional Support: Chronic pain and limited mobility can take a toll emotionally. Caregivers provide essential companionship and emotional reassurance.
Fall Prevention: Families can assist in modifying the home environment to reduce fall risks, such as installing grab bars or ensuring that pathways are clear.
Advocacy: Caregivers can advocate for the patient, ensuring they have access to necessary treatments and healthcare resources.
Support from loved ones is crucial to enhancing a patient's quality of life and aiding in their recovery.
Innovations in Bone Health Research
Research in metabolic bone disorders has led to exciting innovations aimed at improving treatment and understanding the underlying causes of these conditions.
Stem Cell Therapy: Research into stem cells offers potential treatments for regenerating bone tissue and correcting bone loss in severe cases of osteoporosis and Paget’s disease.
Genetic Therapy: Advancements in genetic research are helping to identify genetic mutations associated with bone diseases, offering the possibility of personalized treatments in the future.
New Medications: Scientists are developing new drugs that can stimulate bone formation, halt bone resorption, and even target specific biochemical pathways involved in bone metabolism.
Bone Regeneration Techniques: Researchers are exploring ways to stimulate bone regeneration through bioengineered scaffolds or proteins that can enhance bone healing.
These innovations are paving the way for more effective and targeted treatments for metabolic bone disorders in the future.
Conclusion
Metabolic bone disorders are complex conditions that require a multifaceted approach to treatment. With the right interventions, including medications, lifestyle changes, and support systems, individuals with these disorders can live full and active lives.
Early Diagnosis is Key: Timely detection through bone density testing and blood work can prevent serious complications, such as fractures and deformities.
Ongoing Management: Treatment doesn’t stop after initial care. It requires regular follow-ups, a balanced diet, exercise, and medication to keep the disease in check.
Patient Empowerment: Knowledge is power. Patients should stay informed about their condition, ask questions, and actively engage in their treatment plan to achieve the best possible outcomes.
By adopting a comprehensive treatment plan and working closely with healthcare providers, people with metabolic bone disorders can manage their conditions effectively and improve their quality of life.