Introduction
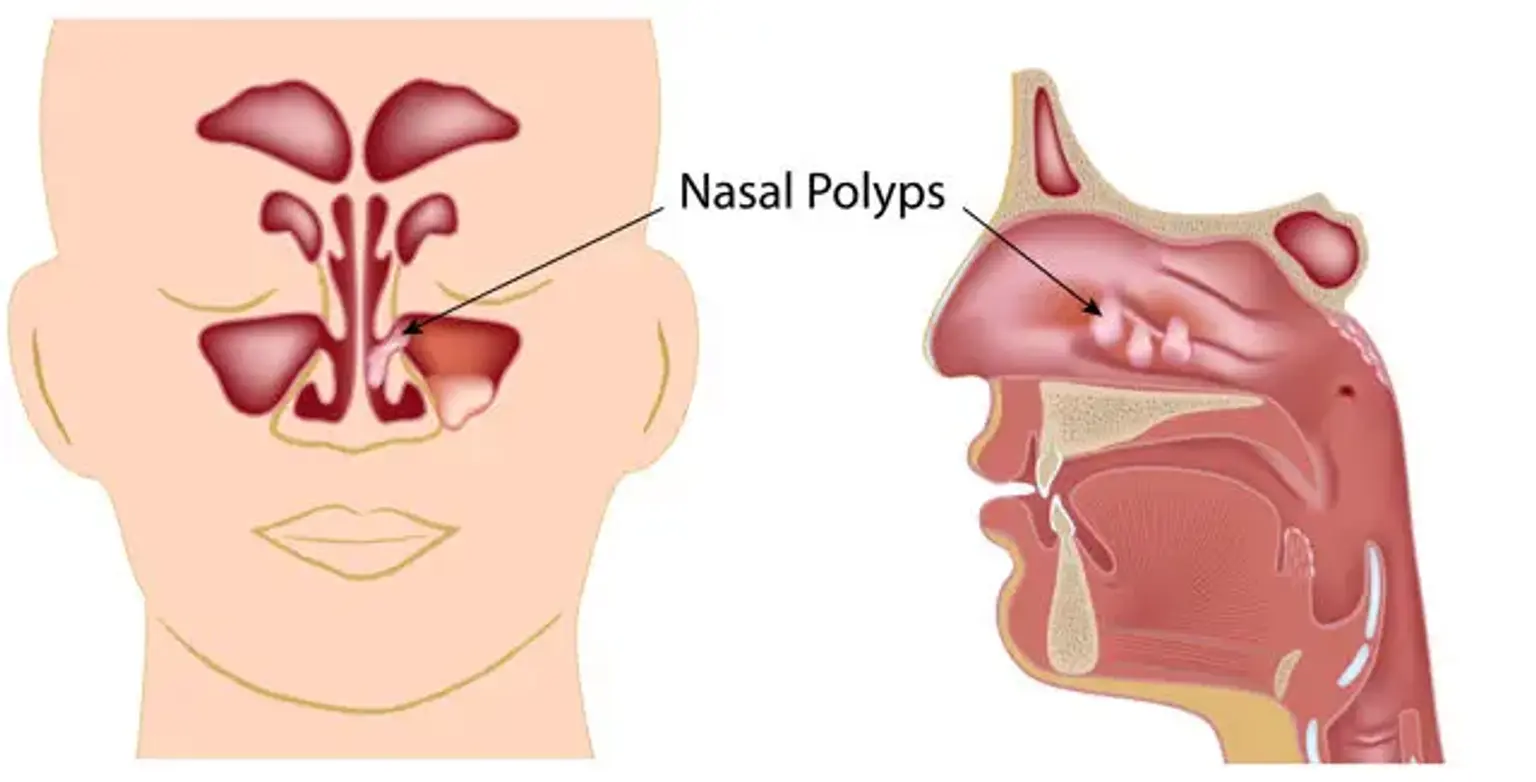
Nasal polyps are noncancerous growths that form inside the nasal passages or sinuses, often as a result of chronic inflammation. These growths can block airflow and make it harder to breathe through your nose, leading to symptoms like nasal congestion, difficulty smelling, and sinus pressure. Though they may be small initially, untreated nasal polyps can grow and cause persistent discomfort.
Treatment for nasal polyps is essential to relieve symptoms, improve breathing, and prevent the condition from worsening. Options range from medications like nasal sprays and corticosteroids to surgical procedures for larger or recurrent polyps. Understanding your treatment options can help you manage the condition effectively and restore your quality of life.
What Are Nasal Polyps?
Nasal polyps are soft, painless growths that develop from the lining of your nasal passages or sinuses. They are typically associated with long-term inflammation, often due to conditions like chronic sinusitis or allergic rhinitis. Polyps can vary in size from small, seed-like structures to larger, more obstructive masses that block airflow.
The exact cause of nasal polyps is not fully understood, but they are believed to develop when the mucous membranes inside the nose and sinuses become inflamed over time. Inflammation causes the tissue to swell, eventually forming polyps. While anyone can develop nasal polyps, they are more common in people with asthma, allergies, or other chronic respiratory conditions.
Symptoms of Nasal Polyps
The most common symptoms of nasal polyps include:
Nasal congestion: Difficulty breathing through the nose due to blocked nasal passages.
Loss of smell or taste: Polyps can obstruct the sense of smell, making food and environmental scents less noticeable.
Facial pressure or pain: The buildup of mucus and pressure in the sinuses can cause discomfort, especially around the eyes or forehead.
Frequent sinus infections: Blocked sinuses create a breeding ground for bacteria, leading to recurring infections.
In some cases, nasal polyps may cause snoring, a post-nasal drip, or a reduced sense of taste. If left untreated, the symptoms can worsen, affecting your quality of life and ability to function day-to-day.
Risk Factors for Developing Nasal Polyps
Several factors can increase the risk of developing nasal polyps:
Chronic sinusitis: People with chronic inflammation in the sinuses are more likely to develop polyps.
Allergic conditions: Conditions like asthma, hay fever, and allergic rhinitis are commonly associated with nasal polyps.
Cystic fibrosis: This genetic condition often causes chronic sinus infections and polyps to develop in the nasal passages.
Family history: A family history of nasal polyps can increase your likelihood of developing them.
Exposure to irritants: Environmental factors such as tobacco smoke, air pollution, or chemical irritants can contribute to nasal inflammation and polyps.
Understanding these risk factors can help in early detection and treatment of nasal polyps, allowing for better management and prevention of complications.
Non-Surgical Treatments for Nasal Polyps
Most nasal polyps can be managed with medications before surgery is considered. Common treatments include:
Steroid nasal sprays: These are often the first line of treatment, reducing inflammation and shrinking the polyps. Examples include fluticasone and mometasone. They help alleviate congestion and improve breathing.
Oral corticosteroids: In severe cases, doctors may prescribe oral steroids like prednisone to reduce inflammation. However, these are typically used for short-term treatment due to potential side effects.
Saline nasal irrigation: Using a saline solution to rinse the nasal passages can help clear mucus, reduce irritation, and relieve congestion.
Decongestants: These can temporarily relieve nasal blockage, but they’re not recommended for long-term use due to possible side effects.
Medical Diagnosis of Nasal Polyps
To diagnose nasal polyps, a doctor will typically start with a physical exam, during which they will inspect the inside of your nose using a nasal speculum. If polyps are suspected, your doctor may perform a nasal endoscopy, a procedure where a thin tube with a camera is inserted into the nose to get a clear view of the polyps.
In some cases, imaging tests like a CT scan or MRI may be recommended to assess the size and extent of the polyps, especially if surgery is being considered. Proper diagnosis is important for tailoring the most effective treatment plan.
Steroid Nasal Sprays: The First Line of Treatment
Steroid nasal sprays are often the first treatment prescribed for nasal polyps. These sprays work by reducing inflammation and shrinking the polyps over time. They are easy to use and effective for many patients.
Popular steroid nasal sprays include fluticasone, budesonide, and mometasone. These sprays are typically safe when used as directed but can cause mild side effects like nasal dryness or irritation. It’s important to follow your doctor’s instructions and continue using the spray consistently for the best results, even if symptoms start to improve.
Endoscopic Sinus Surgery: A Closer Look
Endoscopic sinus surgery is the most common and effective surgical treatment for nasal polyps. It involves the use of a tiny camera (endoscope) and specialized instruments to remove polyps and clear blocked sinuses. The surgery is minimally invasive, meaning it requires only small incisions inside the nostrils, reducing recovery time and scarring.
This procedure is typically done under general anesthesia and can be completed in less than two hours. After surgery, most patients experience significant relief from symptoms like congestion and facial pressure. However, it's important to understand that while surgery can remove the polyps, it doesn't prevent them from coming back, so long-term management with medications may still be necessary.
Aftercare and Recovery from Nasal Polyp Surgery
Recovery from nasal polyp surgery usually takes about one to two weeks. During the first few days, patients may experience mild discomfort, including congestion, drainage, or a stuffy nose. Doctors typically recommend saline nasal irrigation and steroid nasal sprays to keep the nasal passages clear and reduce swelling.
It’s important to avoid strenuous activities, including heavy lifting or bending over, for several weeks to prevent complications. Most patients can return to work or school within 7–10 days, but complete healing may take several months, especially if the sinuses were severely blocked. Regular follow-up visits with your doctor will be necessary to monitor healing and detect any recurrence of polyps.
Managing Nasal Polyps Long-Term
Even after surgery or medication, nasal polyps can recur. Long-term management involves a combination of lifestyle changes and ongoing treatments. Regular use of steroid nasal sprays is common, as they help keep inflammation in check and prevent new polyps from forming.
In addition to medication, patients should try to avoid known triggers like allergens, irritants, and pollutants. Maintaining good sinus hygiene, using saline irrigation, and addressing underlying conditions like allergies or asthma can help manage nasal polyps in the long run. Your doctor may also recommend periodic CT scans to monitor the condition of your sinuses.
Surgery for Nasal Polyps: When Is It Necessary?
When medications fail to reduce polyps or if polyps keep recurring, surgery may be necessary. The most common surgical option is endoscopic sinus surgery, which is minimally invasive and performed under general anesthesia.
During the procedure, a small camera and specialized instruments are inserted into the nasal passages to remove the polyps and clear blocked sinuses. Endoscopic surgery typically results in less pain and quicker recovery compared to traditional surgery. However, while the procedure is effective, it doesn’t guarantee that the polyps won’t return, which is why ongoing treatment may still be required.
Lifestyle Changes and Natural Remedies for Nasal Polyps
In addition to medical treatments, certain lifestyle changes and natural remedies can help alleviate symptoms of nasal polyps and improve overall sinus health. These include:
Humidifiers: Keeping the air moist can help reduce dryness and irritation in the nasal passages, especially in dry climates.
Diet adjustments: Some people find that certain foods, such as dairy or processed foods, can worsen inflammation. A diet rich in fruits, vegetables, and anti-inflammatory foods may help reduce swelling in the sinuses.
Essential oils: Inhaling steam infused with essential oils like eucalyptus or peppermint may provide temporary relief from congestion and open up blocked nasal passages.
While these natural remedies can complement medical treatments, they should not replace prescribed medications or surgery if needed. Always consult your doctor before trying new treatments to ensure they are safe and effective for your condition.
Risks and Complications of Nasal Polyp Treatments
While most treatments for nasal polyps are effective, they come with potential risks and complications. For medications, long-term use of corticosteroids can lead to side effects such as nasal irritation, headaches, or thinning of the skin. Oral corticosteroids, while effective in reducing inflammation, can cause more serious side effects like weight gain, high blood pressure, and weakened bones if used for extended periods.
For surgery, while endoscopic sinus surgery is minimally invasive, complications can still occur. These include bleeding, infection, or injury to the surrounding tissues, such as the eyes or brain. In rare cases, the polyps may return even after successful surgery. That’s why it’s important to follow post-surgical care instructions and continue regular checkups to monitor for recurrence.
Cost and Insurance Coverage for Nasal Polyp Treatment
The cost of treating nasal polyps can vary widely depending on the treatment method. Steroid nasal sprays are generally affordable, though ongoing use may become expensive over time. Oral corticosteroids and other medications may also add up in cost, particularly if long-term treatment is required.
For surgery, the cost can be significant. Endoscopic sinus surgery may cost several thousand dollars, depending on the complexity of the procedure and the healthcare provider. However, most insurance plans cover the cost of surgery and medications for nasal polyps, as it is often considered medically necessary. It’s important to check with your insurance provider to understand your coverage and any out-of-pocket expenses.
If cost is a concern, there may be financial assistance programs or payment plans available, especially for those who do not have adequate insurance coverage.
The Role of Allergies in Nasal Polyps
Allergic reactions play a significant role in the development of nasal polyps. People with conditions like allergic rhinitis or asthma are at an increased risk of developing polyps due to chronic inflammation in the nasal passages. Allergies cause the immune system to release chemicals that trigger inflammation in the nasal passages, leading to the growth of polyps.
Managing allergies is a key part of preventing and treating nasal polyps. Antihistamines, nasal corticosteroids, and allergy shots (immunotherapy) can help reduce allergic reactions and the inflammation that leads to polyp formation. In addition, avoiding allergens—such as pollen, dust, and pet dander—can help reduce the risk of polyps developing or recurring.
Polyp Recurrence: Prevention and Management
Even after successful treatment, nasal polyps can return. This is why ongoing management is crucial. After surgery or medication, regular use of steroid nasal sprays is often recommended to keep inflammation under control and prevent polyps from regrowing. In some cases, doctors may suggest using saline nasal irrigation daily to keep the sinuses clear and reduce irritation.
Other preventive measures include avoiding triggers like allergens, cigarette smoke, and air pollutants, which can aggravate sinus inflammation. For those with underlying conditions like asthma or allergies, managing these conditions with appropriate medication is also vital in reducing the risk of polyp recurrence. Regular follow-up appointments with your doctor can help detect early signs of recurrence, allowing for prompt treatment.