Pacemaker Implantation
Overview
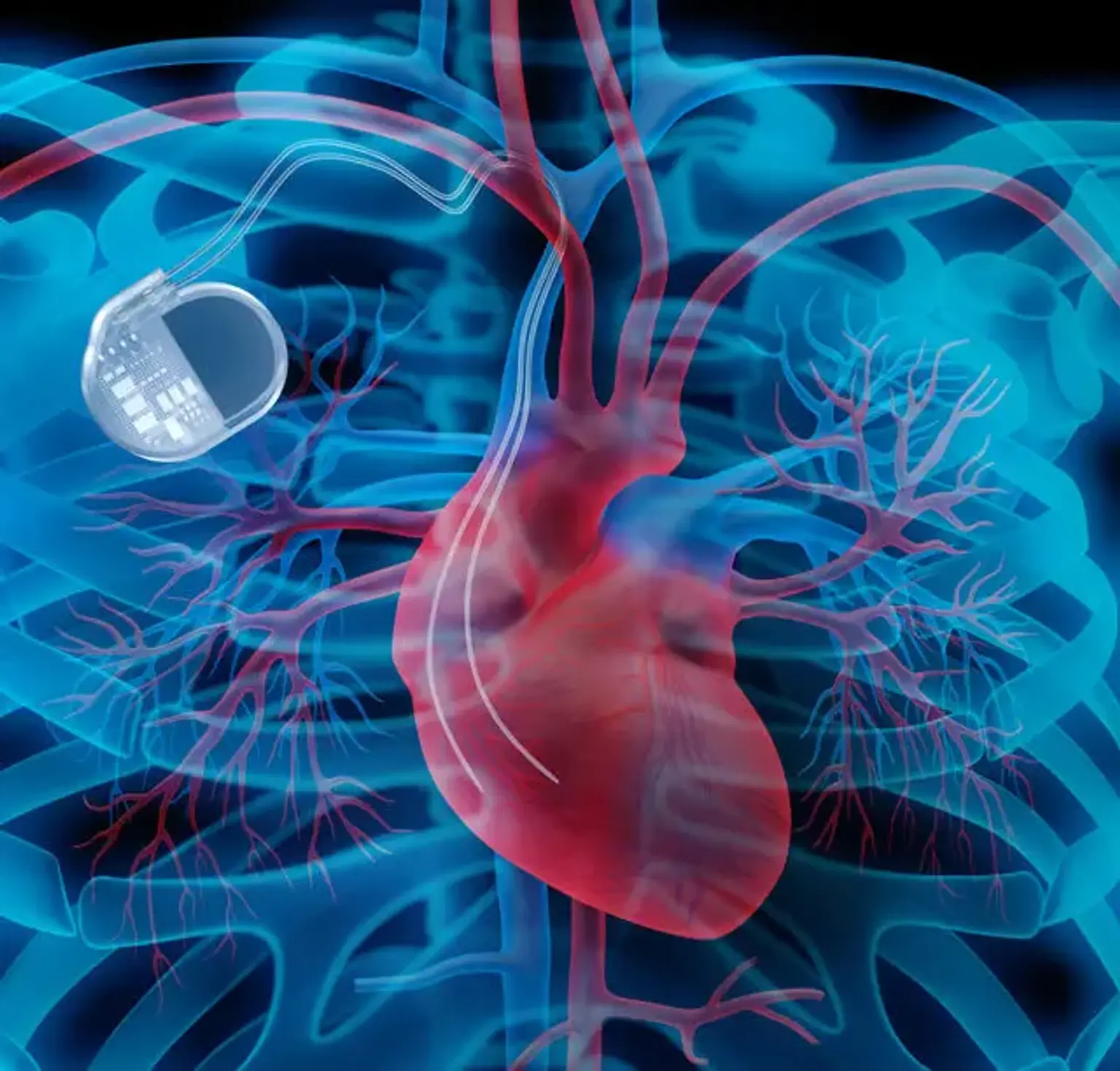
A pacemaker (PM) is a medical device that regulates the heart's beating by using electrical impulses given by electrodes contracting the heart muscles. The basic function of this device is to maintain an adequate heart rate, either because the heart's natural PM is insufficient or because there is a block in the electrical conduction system.
Modern pacemakers are externally programmable, allowing the cardiologist to choose the best pacing settings for particular patients. Some implanted devices combine a PM with a defibrillator. PMs can be either transitory or long-term.
Temporary PMs are used to treat short-term cardiac disorders including a sluggish heartbeat induced by a heart attack, heart surgery, or a medication overdose. Permanent PMs are used to treat chronic cardiac rhythm disorders. Some arrhythmia symptoms, such as exhaustion and fainting, can be relieved by a PM. A PM can also assist a person with abnormal HRs in resuming a more active lifestyle.
Pacemaker definition
The origin of the pacemaker idea may be traced back over 200 years. Luigi Galvani found in the late 1700s that he could force a frog heart to contract merely by putting an electrical current through it. This hypothesis was further realized over 100 years later when Guilliame de Boulogne used electricity to successfully resuscitate an infant. He was able to do so by applying an electrical current to the patient's chest via a return electrode on the patient's leg following a drowning.
Pacemakers are artificial electrical pulse generators that release a pulse with a length of 0.5 to 25 milliseconds and an output voltage of 0.1 to 15 volts at a frequency of up to 300 times per minute. Whether the device is temporary or permanent, the cardiologist or pacemaker technician will be able to interrogate and regulate the pacing rate, pulse width, and voltage.
Pacemakers are normally classified as either external or internal. Almost typically, the external variant is used to temporarily stabilize the patient or to assist some form of surgical treatment. The implanted variety is generally permanent and far more sophisticated than the temporary, external form.
Pacemakers are one form of implanted cardiac electrical device (known as CIED). Implantable cardioverter-defibrillators are also included in this wide category (ICDs). This class of devices was originally presented in the 1950s, shortly after the transistor was invented. The pacemaker device has evolved along with technology. The first implanted ICD was produced in 1980, and it has grown increasingly difficult to distinguish between pacemakers and ICDs since then.
This is due to the fact that every ICD currently implanted has an anti-bradycardia pacing feature. To avoid unneeded ICD therapy, it is vital for the patient and any health care professional to understand which device has been placed. This is most likely to happen with any electromagnetic interference (EMI) and might result in the gadget being activated (if it is an ICD). The majority of CIEDs employ numerous insulated lead wires with non-insulated tips that are implanted in the heart by percutaneous vein insertion or directly by a cardiac surgeon. Cardiac pacemakers are composed of two components: the pulse generator and the leads or electrodes.
Epidemiology
There is no simple way to calculate the total number of implanted cardiac devices in the United States and throughout the world today. Various sources indicate that there are between 500,000 and 3 million people in the United States who have an implanted pacemaker. The likelihood of pacemaker insertion rises considerably with age.
In fact, individuals over the age of 65 account for more than 70% of all pacemaker implants. With an aging population and rising life expectancy, the number of ICDs may only rise tremendously in the future. Over 3000 pacemaker types have been introduced in the United States alone since their introduction in the 1950s.
Etiology
The American College of Cardiology (ACC), American Heart Association (AHA), and Heart Rhythm Society (HRS) have collaborated to develop national recommendations for the implantation of artificial cardiac pacemakers. The scope of this article does not allow for a comprehensive examination of these rules, but an outline will be provided. The following are the primary indications for pacemaker implantation:
- Symptomatic bradycardia from sinus node disease
- Symptomatic bradycardia from atrioventricular node disease
- Long QT syndrome
- Hypertrophic obstructive cardiomyopathy
- Dilated cardiomyopathy
- During AV node ablation
- Cardiac resynchronization therapy with biventricular pacing
- Advanced 2nd or third-degree heart block
- Recurrent syncope
Pacemakers are now programmed non-invasively. Pacemaker generators include an x-ray code that may be seen on a chest x-ray.
Pathophysiology
Patients who require permanent pacemaker implantation frequently exhibit symptoms such as dizziness, lightheadedness, weariness, syncope, or a lack of activity tolerance. These symptoms are frequently caused by bradyarrhythmias, and patients will have sinus node dysfunction or atrioventricular (AV) conduction abnormalities.
A comprehensive history, as well as a physical exam, are required to identify whether these symptoms are connected to bradycardia episodes. An EKG and a loop recorder monitor are also critical measures in determining if a permanent pacemaker should be implanted.
Implantation Guidelines
Pacemaker implantation recommendations are provided for children, adolescents, and individuals with congenital cardiac disease, and particular cases are covered below. It is sometimes beneficial to go through the adult sections of the paper. With each successive set of recommendations, there has been a gradual shift toward less stringent signals. Individual judgments are frequently necessary within the framework of the document.
Class I (Pacing is good, useful, and effective, according to evidence and/or widespread agreement.)
- Atrioventricular block of the second or third degree, accompanied by symptomatic bradycardia, ventricular dysfunction, or poor cardiac output.
- Symptoms of sinus node dysfunction during age-inappropriate bradycardia. Bradycardia is defined differently depending on the patient's age and predicted heart rate.
- Advanced second- or third-degree atrioventricular block that does not resolve or continues for at least 7 days following cardiac surgery.
- Congenital third-degree atrioventricular block with a broad QRS escape rhythm, complicated ventricular ectopy, or ventricular malfunction
- Congenital third-degree atrioventricular block in a newborn with a ventricular rate of fewer than 50–55 beats per minute or congenital heart disease with a ventricular rate of less than 70 beats per minute.
- Sustained pause-dependent ventricular tachycardia with or without extended QT, in which the effectiveness of pacing is well demonstrated.
Class II (conditions for which there is conflicting evidence and/or a divergence of opinion)
Class IIa (weight of evidence favours pacing)
- Bradycardia-tachycardia syndrome requiring long-term antiarrhythmic therapy other than digitalis.
- Congenital third-degree atrioventricular block after the first year of life, with an average heart rate of fewer than 50 beats per minute, sudden pauses in ventricular rate two or three times the basic cycle duration, or indications of chronotropic incompetence.
- Long-QT syndrome accompanied by 2:1 or third-degree atrioventricular block.
- Asymptomatic sinus bradycardia in a kid with complicated congenital heart disease, defined as a resting heart rate of fewer than 40 beats per minute or ventricular rate pauses lasting more than 3 seconds.
- Patients with congenital heart disease who have poor haemodynamics as a result of sinus bradycardia or lack of atrioventricular synchronization.
Class IIb (evidence for pacing is less well established)
- Transient third-degree atrioventricular block that reverts to sinus rhythm with persistent bifascicular block after surgery.
- Congenital third-degree atrioventricular block with a tolerable rate, thin QRS complex, and adequate ventricular function in an asymptomatic newborn, child, teenager, or young adult.
- Asymptomatic sinus bradycardia in a teenager with congenital heart disease, with a resting heart rate of fewer than 40 beats per minute or ventricular rate pauses of more than 3 seconds.
- Neuromuscular illnesses with any degree of atrioventricular block (including first-degree atrioventricular block), with or without symptoms, since atrioventricular conduction disease can proceed in an unanticipated manner.
Class III (pacing not indicated)
- Transient post-operative atrioventricular block with return of normal atrioventricular conduction.
- Asymptomatic post-operative bifascicular block with or without first-degree atrioventricular block.
- Asymptomatic type I second-degree atrioventricular block.
- Adolescent sinus bradycardia with a longest RR interval of less than 3 seconds and a minimum heart rate of more than 40 beats per minute.
Technique of implantation
Cefazolin 1 g or patient weight-based dose is usually given intravenously (IV) one hour before the surgery. If the patient is allergic to penicillins or cephalosporins, 1 g IV vancomycin or another suitable antibiotic may be given prior to surgery.
- Venous access
A percutaneous technique is used to reach a central vein (such as the subclavian or axillary vein). In patients whose access is technically problematic due to distorted bone landmarks, a quick fluoroscopic assessment will considerably decrease the time and problems involved with establishing access.
The subclavian vein is normally accessible at the first rib and clavicle junction. On occasion, phlebography may be necessary to adequately view the vein or to establish its patency. Some facilities use the first rib approach under fluoroscopy, with no or little pneumothorax.
Following venous access, a guide wire is advanced through the access needle, with the tip of the guide wire positioned in the right atrium or vena caval region under fluoroscopy. The needle is then removed, but the guide wire remains in place. If indicated, a second access will be acquired in the same manner for the placement of a second guide wire.
A double-wire technique is sometimes used, in which two guide wires are inserted through the first sheath and the sheath is then withdrawn, allowing two separate sheaths to be advanced over the two guide wires. During sheath or lead advancement, this approach may generate some resistance or friction.
- Creation of pocket
In the infraclavicular region, a 1.5- to 2-inch incision is made parallel to the middle third of the clavicle, and a subcutaneous pocket is established by sharp and blunt dissection where the pacemaker generator will be installed. Some surgeons prefer to create the pocket first and then get access through the pocket or through venous cutdown; after access is gained, the guide wires are positioned as described above.
- Placement of lead(s)
A unique peel-away sheath and dilator are advanced over the guide wire. The guide wire and dilator are removed, but the sheath remains in place. A stylet (a thin wire) is put within the central channel of the pacemaker lead to stiffen it, and the lead-stylet combination is then inserted into the sheath and progressed to the proper heart chamber under fluoroscopy. The ventricular lead is usually placed ahead of the atrial lead to prevent it from being dislodged.
Making a small curve at the tip of the stylet makes the ventricular lead tip more maneuverable, allowing it to be placed more easily across the tricuspid valve and at the right ventricular apex or septum. Positioning techniques for the ventricular lead have been reported.
Once the right lead location has been determined, the lead is attached to the endocardium either passively with tines (similar to a grappling hook) or actively using a helical screw situated at the tip. The screw at the pacemaker's tip is extended or retracted by rotating the outer end of the lead with a torque device. Fluoroscopy is used to ensure if the screw has been properly extended. Each manufacturer has its own distinctive identifying markings for ensuring proper screw extension.
After securing the lead in place, the introduction sheath is carefully peeled away, leaving the lead in situ. After the pacing lead stylet is removed, the pacing and sensing thresholds, as well as lead impedances, are monitored using a pacing system analyzer, and pacing is done at 10 V to ensure that diaphragmatic stimulation is not caused. After the lead location and thresholds have been confirmed, the proximal end of the lead is fastened to the underlying tissue (ie, pectoralis) with a nonabsorbable suture sewed to a sleeve situated on the lead.
If a second lead is indicated, it is inserted via a second sheath into the right atrium, with the lead tip generally inserted into the right atrial appendage using a premade J-shaped stylet.
The lead can be placed medially or lateral free wall of the right atrium in a patient who does not have an atrial appendage as a result of previous cardiac surgery. The atrial lead location is verified, impedance is evaluated, the stylet is removed, and the lead is attached to the underlying pectoralis with a nonabsorbable suture, as with the ventricular lead.
- Positioning of pulse generator
The pacemaker pocket is irrigated with antimicrobial solution after the leads have been appropriately positioned, tested, and sutured to the underlying tissue, and the pulse generator is firmly linked to the leads. To prevent migration or twiddler syndrome, many doctors use a nonabsorbable suture to bind the pulse generator to the underlying tissue.
The pacemaker is often placed superficial to the pectoralis, however a subpectoral or inframammary placement is occasionally necessary. After confirming hemostasis, a last examination under fluoroscopy before closing the incision is recommended to ensure proper lead location.
- Completion and closure
Absorbable sutures and sticky strips are used to seal the wound in layers. The incision surface is covered with a sterile dressing. To limit mobility, an arm restraint or immobilizer is put to the unilateral arm for 12-24 hours.
Typically, a postoperative chest radiograph is taken to check lead location and rule out pneumothorax. Posteroanterior and lateral chest radiographs will be obtained again before release the next day to check lead locations and rule out delayed pneumothorax.
After the treatment, pain levels are normally modest, and the patient might be given pain medication to address breakthrough discomfort related with the incision site.
Follow up following pacemaker insertion
There are no clear guidelines for adequate follow-up after pacemaker insertion. In terms of pacemaker evaluation, battery state, and stimulation and sensing thresholds, there is a wide range of follow-up. More importantly, studies reveal that pacemaker reprogramming is frequently disregarded in the long run, making the pacemaker visit unnecessary.
Although nurses do not implant pacemakers, they are critical in examining the preoperative and postoperative health of patients having pacemaker implantation. Advanced practice nurses now evaluate patients in preoperative clinics and play an important role in teaching patients and families about pacemaker care and follow-up.
Another important component is the pharmacist's handling of drugs in patients with pacemakers. The choice to discontinue anticoagulation and begin beta-blockers before to surgery should always be taken in conjunction with a cardiologist. Only by stratifying risk in the preoperative phase and doing medication reconciliation can patients receive appropriate treatment following pacemaker implantation.
- Outcomes
The short-term results for pacemaker insertions are favorable, but the long-term outcomes depend on a variety of circumstances. The mortality rate after pacemaker implantation ranges from 1-4 percent, with problems occurring in 4-15 percent of patients. The presence of renal failure, a high NYHA class, a poor ejection fraction, a low platelet count, stroke, and body mass index are all factors that influence mortality and complications. Given the high morbidity of pacemakers, an interprofessional team of healthcare workers that constantly monitor the patient and make early referrals may help reduce issues.
Complications
From 1993 to 2009, 2.9 million patients in the United States obtained a primary PM. Although PM implantation is a minimally invasive treatment, problems might occur during or after the surgery. The rate of early complications is 4-5 percent, and the rate of late complications is 2.7 percent; however, these rates can be presented within a wider range in literature due to difficulties in defining and identifying complications in different studies, which could raise the rate up to 12.6 percent.
The combination of technology advancement and growing operator expertise has resulted in a considerable reduction in the occurrence of difficulties. These problems are classified as early (postoperative, during hospitalization, and within 30 days) and late [in literature, short-term complications are also defined as those that occur within 3 months, according to implantation time, and also procedure- and device-based, as shown in tables].
Complications associated to venous access (e.g., pneumothorax), leads (e.g., lead dislodgement), and the generator pocket (e.g., hematoma) are classified as serious (e.g., mortality, heart perforation) and minor (e.g., hematoma) (e.g., drug reaction, hematoma). Mortality is uncommon, occurring at a rate of 0.08-1.1 percent. Complications connected to the implantation technique, such as lead dislodgement and pneumothorax, are the most common.
Dual chamber device implantation may be more difficult; nonetheless, the difference in complication rates between single and complex pacing is not constant across studies, most likely because to differences in technology and operator skill.
Lead dislodgement is the most frequent consequence (atrial dislodgement is more prevalent than ventricular dislodgement), followed by pneumothorax, infection, bleeding/pocket hematoma, and heart perforation, but necessarily in that order, according on the research.
Pacemaker device infection
Cardiac device infections can result in longer hospital stays, greater expenditures, and a higher mortality rate. If they are recognized and treated early, device extraction can be avoided, and patient morbidity and death can be considerably decreased.
Pacemaker infections may be divided into 2 general types on the basis of the initial source of infection:
- Primary infections occur when the device or pocket itself becomes infected, generally as a result of contamination during the implantation process.
- Secondary infection – Bacteremia from a separate source seeds the leads, device, and pocket.
The overall infection rate of medical devices ranges from 0.68 to 2.2 percent. There are independent risk factors for cardiac device infection. These are some examples:
- Pulse generator replacement
- Dual- or triple-chamber device implantation
- Advanced patient age (older than 60 years)
- Renal dysfunction
- Oral anticoagulation
Current treatment for device infection includes complete device system extraction (either percutaneously or intraoperatively), antimicrobial therapy of suitable length, and reimplantation of a replacement pacing system at a different location. In certain infected individuals, implanting a leadless permanent pacemaker lead (Micra, Medtronic Inc) may be desirable. The vast majority of individuals who get such therapy will be clear of infection.
Conclusion
A pacemaker insertion is the placement of a tiny electronic device in the chest to assist manage sluggish electrical abnormalities with the heart. A pacemaker may be advised to guarantee that the heartbeat does not slow to an unsafely low rate.
Taking actions to enhance your health and fitness, such as quitting smoking if you smoke, eating a nutritious diet, and exercising on a regular basis, should help you recover faster and lessen the chance of problems.
During the preoperative evaluation, you will normally be instructed when you must cease eating or drinking before surgery.