Percutaneous Coronary Intervention
Coronary artery disease, or CAD, is a type of heart disease that can be managed with drugs as well as dietary and lifestyle modifications. In the event that your situation worsens, your doctor may recommend percutaneous coronary intervention, or PCI, to treat your heart arteries.
Procedures to open occluded coronary arteries, blood vessels that give oxygen to your heart muscles via blood, are referred to as percutaneous coronary intervention.
Plaque, which is made up of fatty materials like cholesterol, can build up in these arteries, leaving them stiff and narrow, restricting blood flow and leading to coronary artery disease (CAD).
Heart damage, chest pain, difficulty breathing, fatigue, and an increased risk of heart attack can all be symptoms of poor blood flow to the heart. With time, your heart can deteriorate, which can result in heart failure.
Percutaneous coronary intervention (PCI) is a procedure that treats and relieves the symptoms of coronary artery disease (CAD), such as chest pain. It can also help prevent cardiac damage during or after myocardial infarction.
Percutaneous Coronary Intervention (PCI)
Percutaneous Coronary Intervention (PCI), also known as coronary angioplasty or stenting, is a treatment for treating narrowing or blockage in the arteries that feed blood to the heart.
The heart is a muscular organ that pumps oxygen-rich blood throughout the body, allowing the organs and muscles to function properly. In order to function properly, the heart needs a steady flow of oxygen. This is delivered to the heart via the coronary arteries (blood vessels) in the bloodstream.
These arteries can narrow or obstruct as a result of fatty material accumulating within the arterial wall (atherosclerosis), causing them to narrow or become completely blocked. This effectively reduces blood supply to the heart, resulting in angina and heart attacks. Coronary artery disease is the medical term for this.
Where Does Percutaneous Coronary Intervention Take Place?
The practice takes place in a specialized theater called the catheter laboratory. There is a lot of technology in the catheter laboratory, including a bed or theater table with big x-ray cameras above it. During the procedure, these cameras move around the bed, and the table may need to be moved on occasion.
You'll notice that some sections of the equipment come close to your chest and head on occasion, but they won't contact you. The doctor will be able to receive clear pictures of your heart and coronary arteries as a result of this. The less radiation you are exposed to throughout the procedure, the closer the equipment is to you.
During the procedure, a team of roughly 6 healthcare professionals works in the catheter laboratory. A cardiac physiologist, one or two doctors, two nurses, a radiographer (x-ray specialist who operates the cameras and takes the images), and a cardiac physiologist (who monitors your heart rhythm and blood pressure during the procedure) are all part of the team. The staff will be dressed for the occasion and will be wearing lead aprons to protect themselves from radiation. At some points during the procedure, the staff will be asked to leave the theater table. Throughout the procedure, you will hear certain noises from the equipment, such as beeping or buzzing. This is normal, so don't be frustrated.
During the procedure, you will be fully conscious and alert. As a result, you'll hear the team conversing and discussing the procedure in detail. This will include them speaking out loud some technical words and measurements, which is very normal, so don't be scared. During your procedure, images will be collected and recorded, and you should be informed that the specialist may request a lot of equipment from the nursing or technical staff; this is to be expected.
You may be treated in a teaching hospital, there may be junior medical practitioners assisting or in attendance during the procedure, and the doctor may interact with them. Again, it's natural for the doctor to need to concentrate at times and/or discuss with other members of the team.
Types of Percutaneous Coronary Intervention
The basic purpose of PCI is to clear blocked arteries; however, the doctor can do it in a variety of ways. The following are examples of PCI types:
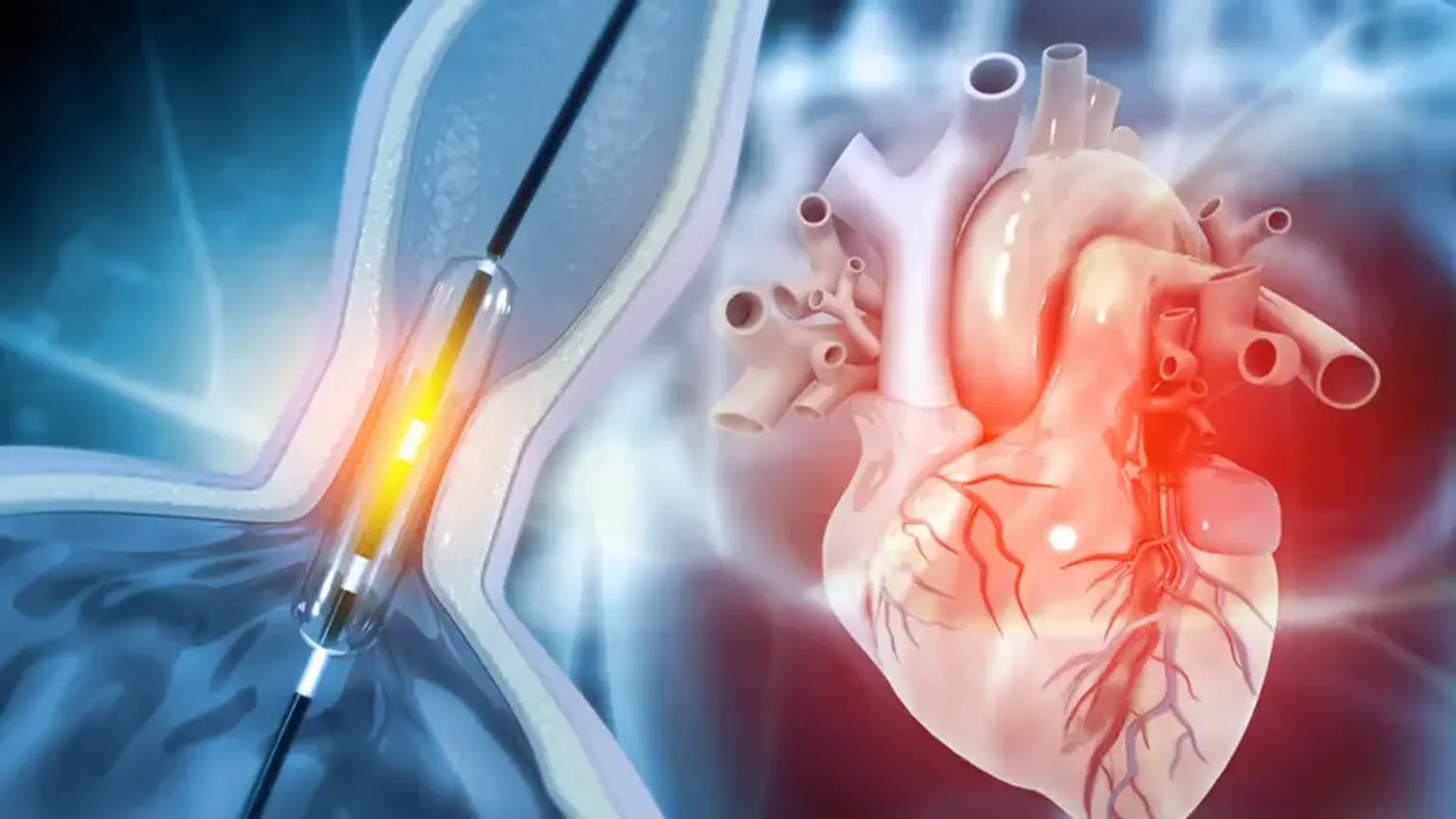
- Balloon angioplasty. A balloon is placed in the artery and expanded to push plaque out of the way.
- Laser angioplasty. Plaque is vaporized using a laser put on the tip of a catheter.
- Rotational atherectomy. To dissolve calcium deposits, a special drill is placed into the artery.
- Angioplasty with a stent. The artery is opened with a balloon, and a permanent metal coil is implanted to help maintain it open.
- Impella-Supported PCI. To aid the heart in pumping blood, a small pump is placed into the heart through the skin.
Percutaneous Coronary Intervention Indications
Percutaneous coronary interventions (PCI) comprise procedures such as percutaneous transluminal coronary angioplasty (PTCA) and stent implantation. The most frequent indications are for the treatment of:
- Acute myocardial infarction (especially in patients with establishing or established cardiogenic shock)
- Angina pectoris (stable or unstable)
- Myocardial ischemia
Transmural ST-segment–elevation myocardial infarction (STEMI) is best treated with PTCA and stent implantation within 90 minutes after the beginning of discomfort. Elective PCI may be useful for patients who have had a myocardial infarction (MI) and have recurrent or inducible angina before being discharged from the hospital, as well as those who have angina and remained symptomatic after medical treatment.
Peripheral artery disease is also treated with percutaneous transluminal angioplasty (PTA).
Percutaneous Coronary Intervention Contraindications
PCI has certain relative contraindications including:
- Coagulation disorders
- All perfusion to the myocardium is provided by a single diseased artery.
- Significant left main coronary stenosis without collateral blood flow from a native vessel or previous bypass graft to the left anterior descending artery
- Diffusely stenosed vessels without focal narrowing
- Hypercoagulable states
- Lack of cardiac surgical support
- Stenosis less than 50%
- Total stenosis of a coronary artery
Although the absence of cardiac surgical backup is sometimes recognized as an absolute contraindication to PCI, many experts believe that when revascularization is required emergently in STEMI, an experienced team in certified catheterization laboratories should move ahead with PCI even if the surgical backup is not present.
Although bypass is usually chosen in patients with significant left main coronary stenosis who do not have collateral flow from a native vessel or a previous bypass graft, PCI is gradually being used in this situation in some patients.
Percutaneous Coronary Intervention Preparation
You might be asked to a pre-admission clinic, where you will know everything you need to know about the procedure and your recovery. The Nurse Practitioner at the pre-admission clinic will also discuss how to maintain a healthy heart and cardiac rehabilitation with you.
Before the procedure, most people will be given adequate antiplatelet medications (blood thinners). You'll get these either at the pre-admission clinic or when you arrive at the hospital for the procedure. Blood clots can form around the new stent; therefore, the medications will help prevent that.
Shave each side of your groin and your right wrist before going to the hospital. Before your procedure, you must take a bath or shower before entering the hospital.
Fasting is not required for the majority of procedures. If and when you must stop eating before the treatment, you will be notified. Until the procedure, you can drink fluids.
Percutaneous Coronary Intervention Procedure
The procedure is commonly done through the wrist or groin blood vessels. During the procedure, you will be conscious and need to lie flat with one cushion. A local anesthetic will be used to numb the skin around the area where the treatment will be conducted. After that, a small incision is made in the wrist or groin. The blood vessel is entered with a sheath (a long thin plastic tube). This remains in place during the treatment and serves as a guide for inserting and guiding catheters and wires up to the heart. It's possible that you'll feel warm, but that's not a problem. On the x-ray monitor, which will be on the left side, the doctor can see the coronary arteries. You will be able to view the pictures yourself if you so desire.
After that, a fine wire is placed through the narrowed section of the artery, and a balloon is passed over this wire and expanded in the narrowing. This compresses the fatty tissue responsible for constriction (also known as atherosclerosis or plaque).
A stent, a tiny stainless steel mesh tube, is placed into the constricted section of the coronary artery. This is placed on top of a balloon that expands and inflates the stent. The stent functions as a scaffolding, keeping the blood vessel open and allowing for adequate blood flow. The stent is then left in place after the balloon is deflated and removed.
In order to ensure that the narrowed portion of the coronary artery is treated appropriately, it is sometimes important to undertake an assessment of how severe the narrowing is. A fine wire with a pressure monitor at its tip is used to do this. The pressure drop is measured by placing the wire beyond the constriction. Adenosine is a medication that doctors sometimes inject to help precisely evaluate the stenosis. This medication may cause some minor adverse effects, which the nurse and doctor will inform you of before you take it.
How Long Does Percutaneous Coronary Intervention Last?
Some procedures include the treatment of clogged arteries, which might be dangerous. The procedure takes around an hour on average, although it can take longer depending on the number of narrowed blood vessels to be addressed. Some procedures need the treatment of clogged arteries, which can be more difficult and time-consuming.
What Happens after Percutaneous Coronary Intervention?
If your operation was conducted on your wrist, you will be given a pressure band to wear after the surgery. If your surgery was done through the groin, the staff will use physical pressure to stop any bleeding. The staff will put a lot of pressure on you and maybe unpleasant. This can be done on the operating table or in the recovery room. Then you'll be transported back to the ward. The nurse who is caring for you will monitor your heart rate and blood pressure as well as the insertion site frequently. Unless you require more investigations, you will be able to eat and drink. If the procedure was done through your groin, you will need to stay in bed for a few hours afterward. The healthcare team will inform you of this.
For a few days after the procedure, you may feel tightness or discomfort in your chest and at the puncture site. Simple analgesics (pain relievers), such as paracetamol, can be used for this. There may be some bruising around the puncture site as well.
Percutaneous Coronary Intervention Complications
The most common risks associated with balloon angioplasty and stent insertion are:
- The risks of cardiac catheterization and coronary angiography such as allergic reactions, bleeding, stroke, heart attack, and even death.
- Adjunctive anticoagulation-induced bleeding
- Distal embolization and thrombosis
- Stent restenosis and thrombosis
- Arterial dissection
PCI has the greatest risk of contrast nephropathy of any angiographic procedure (due to higher contrast load and procedural duration); this risk can be minimized by preprocedural hydration and, in patients with previously established renal insufficiency, possibly by using a nonionic contrast media or hemofiltration.
The risk of death, MI, and stroke is higher with coronary angiography without angioplasty or stenting. The rate of death after PCI varies depending on the patient and technical conditions. Mortality score systems have been introduced to help doctors in determining the risk of death after PCI, and they can be helpful when counseling patients about treatment alternatives (PCI vs medical management alone).
Stent Thrombosis
Stent thrombosis is a total blockage of the stent that can happen at any time:
- Acute stent thrombosis (immediately during or after the procedure)
- Subacute stent thrombosis (within 30 days of the procedure)
- Late stent thrombosis (after 30 days of the procedure)
Stent thrombosis can be caused by insufficient stent inflation or apposition during the procedure, the withdrawal of dual antiplatelet medications (e.g., due to poor adherence, the need for noncardiac operation), or a combination of the two. The stent may, on rare occasions, break up an intracoronary clot (such as those seen in acute MI), which can embolize distally and cause a heart attack. Protection strategies (for example, momentarily blocking blood flow within the artery with a balloon and then aspirating the emboli, or utilizing a small filter distal to the site of PCI to catch emboli) may improve outcome in PCI performed on a previous saphenous vein graft, but they are not commonly used. The risk of acute thrombosis with balloon angioplasty alone is roughly 7% to 10%.
The use of stents has reduced the need for emergent coronary artery bypass grafting after PCI to less than 2%; the rate of acute and subacute thrombosis is less than 2%. Using a drug-eluting stent, on the other hand, raises the risk of late stent thrombosis by roughly 0.5 percent per year for the first three years.
Stent Restenosis
Restenosis is usually caused by collagen deposition and does not appear until many weeks or months following the treatment; it can result in partial or total artery obstruction.
The risk of subacute restenosis is approximately 6 percent with balloon angioplasty alone, and the total restenosis rate is approximately 35 to 45 percent.
The rate of subacute restenosis with stents is less than 1%. The risk of late restenosis with bare-metal stents is 25% to 30%. The use of a drug-eluting stent reduces the incidence of late restenosis by roughly 5% to 10%.
Arterial Dissection
Various abnormal patterns of contrast loading within the coronary arteries are frequently identified quickly as a sign of artery dissection. The dissected portion is frequently reopened by the insertion of a new stent.
Is Percutaneous Coronary Intervention Painful?
During the procedure, you may feel minor irritation at the insertion site (groin or wrist). Because the blood vessels in the arm are so small, the discomfort is most noticeable there. During the operation, it is also typical to have dull pain. If you are uncomfortable, let the nurse in the catheter lab know so that they can help you as needed. While the balloon is being inflated, you may feel mild discomfort or any pain in your chest, comparable to angina symptoms you may have previously encountered. When the balloon is deflated, the pain should subside soon. You must notify the doctor or nursing staff if you experience any pain during or after the treatment. While the catheter is in the artery in your heart, you may notice that your heart skips a beat or makes an extra beat. This is quite acceptable.
Will Percutaneous Coronary Intervention Work?
The procedure is carried out in great numbers all around the world and is generally a big success. However, success rates are lower when an artery is completely occluded. You will be directed to a cardiac rehabilitation center in order to lower your chance of having more narrowing in other parts of your coronary arteries in the future.
You will be counseled on the necessity of following the medication prescribed to you, as well as how you may help prevent future heart disease by adopting a healthy lifestyle that includes eating well and exercising regularly.
Percutaneous Coronary Intervention Alternatives
This is determined by your heart disease, the results of your angiogram (a test that examines the arteries supplying blood to the heart), and the severity of your symptoms. A Percutaneous Coronary Intervention is not appropriate for all patients with coronary artery disease. As an alternative, these patients may be offered coronary artery bypass grafting (CABG). Angina can also be relieved with bypass surgery. Drugs alone may be used to treat those with stable angina symptoms. If alternative treatments are appropriate, they will be shared with you.
When Can I Resume Normal Activities?
You should be ready to return home the same day, however, some patients may need to stay in the hospital overnight. After your therapy, you should not drive for a week. If you drive a vehicle that requires a specific license, you must take a six-week break from driving.
You should take around a week off work, though this will vary based on the type of work you have. For the next 1-2 weeks, avoid carrying heavy objects. Before you go home, this information will be addressed in greater detail with you, and you will be handed a discharge advice leaflet.
Around 5-6 months after the procedure, you will be evaluated in the outpatient department. All patients are sent to a local cardiac rehabilitation program, which may be at the Heart and Chest Hospital or at your local hospital, where you will receive essential advice and information on how to lower your risk of developing more coronary artery disease in the future. Staff at the rehabilitation facility will call you directly following the procedure, generally a few weeks later.
Conclusion
One of the primary causes of death is coronary artery disease (CAD). Percutaneous coronary intervention (PCI) is a minimally invasive, non-surgical therapy that aims to reduce coronary artery stenosis or blockage and increase blood flow to ischemic tissue. The most frequent procedures for accomplishing this are inflating the narrow portion or placing a stent to maintain the artery open.