Introduction
Minimally invasive epidural neuroplasty is a modern medical procedure designed to relieve chronic back and neck pain caused by spinal nerve compression. Unlike traditional spinal surgeries that require large incisions, neuroplasty offers a less invasive alternative that targets the root cause of pain—usually nerve compression or inflammation—by clearing the epidural space around the affected nerves.
This technique has gained global popularity as a safe, effective, and quicker option for patients looking to avoid the risks and long recovery times associated with major surgeries. With advancements in technology, epidural neuroplasty allows patients to experience significant pain relief with minimal downtime, making it a sought-after solution for those suffering from conditions like sciatica, radiculopathy, and spinal stenosis.
Understanding Epidural Neuroplasty
Epidural neuroplasty involves the use of an epidural catheter and a special combination of medications, such as corticosteroids and local anesthetics, to relieve nerve compression in the epidural space of the spine. The procedure works by delivering the medication directly to the affected area, reducing inflammation and alleviating pain caused by pressure on the spinal nerves.
The key difference between this minimally invasive technique and traditional spinal surgeries is that neuroplasty does not involve cutting through muscles, ligaments, or bone. Instead, small incisions or even a needle may be used, which significantly reduces the risk of complications and speeds up recovery. Through real-time imaging like fluoroscopy, doctors can guide the catheter precisely to the target area, ensuring that only the affected region is treated.
How the Procedure Works
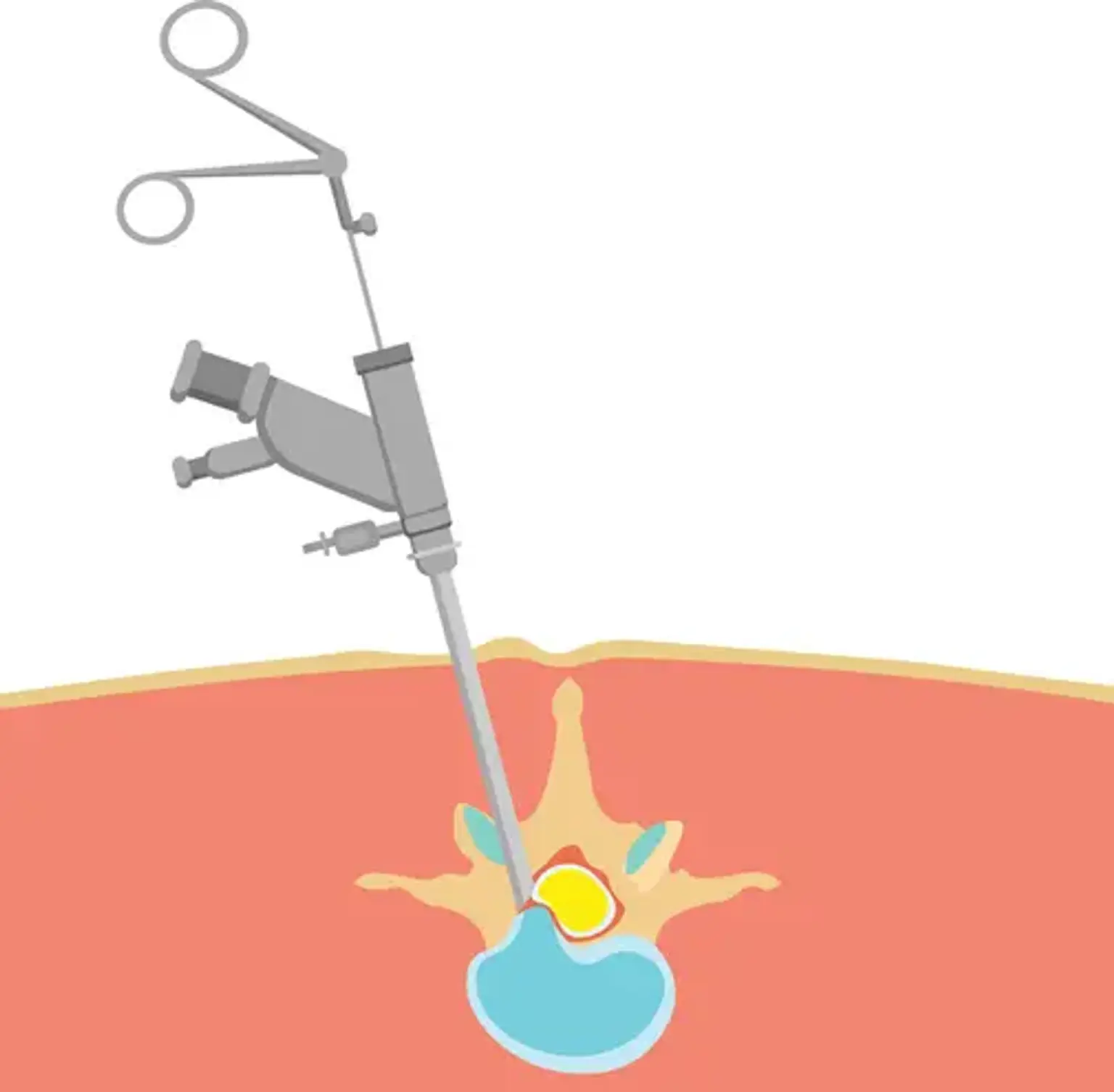
The epidural neuroplasty procedure is minimally invasive, typically performed in an outpatient setting. It begins with the patient being positioned comfortably on the procedure table, usually in a prone (face-down) position. Local anesthesia is administered to numb the skin, followed by the insertion of a needle or catheter into the epidural space, guided by fluoroscopy (real-time X-ray imaging).
Once the catheter is in place, a mixture of medication—typically a combination of steroids and anesthetics—is slowly delivered into the affected area. The medication reduces inflammation, relieves nerve irritation, and decompresses the affected nerve roots. The procedure typically takes about 30 to 60 minutes, and many patients report experiencing immediate pain relief after the treatment.
Because the procedure is minimally invasive, recovery time is much shorter than traditional surgeries, with most patients able to return home the same day and resume normal activities within a few days to a week, depending on their condition.
Minimally Invasive Approach: Benefits and Advantages
One of the main advantages of minimally invasive epidural neuroplasty is that it offers a safer, more efficient alternative to traditional spinal surgery. By using small incisions or a needle, the procedure avoids the need to cut through large muscles and soft tissue, reducing the risk of complications such as infection, excessive bleeding, or nerve damage.
Since the procedure doesn’t require significant cuts or muscle dissection, recovery time is drastically reduced compared to conventional spinal surgeries. Most patients can return home the same day and begin resuming light activities within a few days. Additionally, as it’s an outpatient procedure, patients can avoid hospital stays and their associated costs.
For those dealing with chronic pain, the minimally invasive nature of the treatment provides faster relief, allowing them to regain mobility and improve their quality of life. Many patients experience significant pain relief immediately following the procedure, which can last for weeks or even months, depending on the individual case.
Conditions Treated by Epidural Neuroplasty
Epidural neuroplasty is primarily used to treat conditions caused by nerve irritation or compression, including:
Chronic back pain: Often caused by conditions like herniated discs or spinal stenosis, leading to nerve pressure.
Sciatica: Pain that radiates down the leg due to compression of the sciatic nerve.
Radiculopathy: Nerve root inflammation that causes pain, numbness, or weakness, often due to a herniated disc or spinal stenosis.
Spinal stenosis: Narrowing of the spinal canal, which can compress nerves and cause pain or difficulty in movement.
This procedure can offer relief for patients who have not responded well to conservative treatments like physical therapy, medications, or injections, and it can be particularly beneficial for individuals who wish to avoid the risks of more invasive surgeries.
Effectiveness of Epidural Neuroplasty in Pain Relief
Epidural neuroplasty has been shown to be highly effective in reducing chronic pain, especially in patients with conditions like herniated discs, sciatica, and spinal stenosis. Numerous clinical studies have confirmed its success in providing long-lasting pain relief and improved function.
Research indicates that many patients experience significant improvements in their pain scores, mobility, and overall quality of life following the procedure. In fact, some studies have shown success rates of up to 80-90% for certain conditions, especially in patients who have not responded well to other conservative treatments like physical therapy, pain medications, or epidural steroid injections.
The procedure is also preferred over more invasive surgeries due to its lower complication rates and quicker recovery times. However, it’s important to note that while the results are generally positive, the effectiveness of neuroplasty can vary based on the individual’s condition, the severity of the nerve compression, and other health factors.
Who is a Candidate for Epidural Neuroplasty?
Epidural neuroplasty is typically recommended for patients suffering from chronic pain due to spinal nerve compression who have not found relief from other conservative treatments, such as physical therapy, medications, or standard epidural steroid injections. Ideal candidates are those with conditions like sciatica, radiculopathy, or spinal stenosis, who have not been able to manage their symptoms effectively.
Before undergoing the procedure, patients will need a thorough evaluation by a spinal specialist to assess their medical history, the severity of their condition, and overall health. Candidates should not have significant contraindications such as severe allergies to the medications used during the procedure, active infections, or certain spinal deformities.
Additionally, candidates should be realistic about the potential results. While epidural neuroplasty can provide excellent pain relief, it is not a cure for underlying spinal conditions. It is most effective as part of a broader pain management strategy, including physical therapy and lifestyle changes.
Alternative Treatment Options for Chronic Spinal Pain
While epidural neuroplasty is highly effective for many patients, it is not the only option available for chronic spinal pain. Alternative treatments include:
Physical Therapy: Focuses on strengthening muscles, improving posture, and increasing mobility.
Epidural Steroid Injections: A less invasive injection of corticosteroids to reduce inflammation around the spinal nerves.
Spinal Fusion Surgery: In cases where non-invasive treatments fail, this surgery stabilizes the spine by fusing two or more vertebrae together.
Radiofrequency Ablation (RFA): A procedure that uses heat to interrupt nerve signals responsible for pain.
Each option comes with its own set of benefits and risks, and the best treatment depends on the individual’s condition and personal preferences.
Potential Risks and Complications
Like any medical procedure, epidural neuroplasty carries some risks, although they are rare. Potential complications include infection at the injection site, bleeding, nerve damage, or an allergic reaction to the medication. In very rare cases, the procedure could worsen symptoms or cause temporary discomfort.
To minimize these risks, it’s essential to choose a skilled and experienced spinal specialist who follows strict safety protocols. Prior to the procedure, patients should undergo a thorough evaluation to rule out conditions that could increase the risk of complications.
Patients are advised to follow all post-procedure guidelines carefully and seek medical attention if they notice any unusual symptoms, such as fever, persistent pain, or numbness.
Cost of Minimally Invasive Epidural Neuroplasty
The cost of epidural neuroplasty varies depending on the location, the healthcare provider, and the complexity of the procedure. On average, the procedure can cost between $1,500 and $6,000, though some factors, such as insurance coverage or additional treatments, may influence the final price.
Insurance coverage for epidural neuroplasty can also vary, with some providers covering the procedure if it is deemed medically necessary, especially for patients with conditions like chronic back pain, sciatica, or spinal stenosis. It’s advisable for patients to check with their insurance provider before scheduling the procedure to understand what is covered.
Compared to traditional spinal surgeries, which can cost significantly more and require extended recovery periods, epidural neuroplasty offers a cost-effective solution with fewer associated expenses.
Success Stories: Real-Life Case Studies
Many patients who undergo epidural neuroplasty experience significant improvements in their quality of life. For example, a 45-year-old woman suffering from sciatica for years reported immediate pain relief following the procedure. She was able to return to work within a few days and resume her regular exercise routine after a few weeks of recovery.
Another case involved a 60-year-old man with chronic back pain due to spinal stenosis. After failing to find relief with physical therapy and medication, he opted for neuroplasty and experienced a 70% reduction in pain and increased mobility. He could now enjoy activities he had given up for years, like walking and gardening.
These real-life examples demonstrate the potential of epidural neuroplasty to transform the lives of individuals suffering from chronic spinal pain, offering hope to those who haven't found lasting relief through other treatments.
Global Popularity of Epidural Neuroplasty
Epidural neuroplasty has gained global recognition as a highly effective and minimally invasive treatment for chronic spinal pain. In countries like the United States, Canada, and the United Kingdom, the procedure has become a common alternative to more invasive spinal surgeries. Its success and safety have also led to growing adoption in regions like Europe, Australia, and parts of Asia.
The global appeal of epidural neuroplasty can be attributed to its ability to offer significant pain relief with reduced recovery times. As more patients seek non-invasive treatments, especially those aiming to avoid the risks associated with traditional surgeries, the demand for neuroplasty continues to rise worldwide.
Comparing Epidural Neuroplasty to Other Treatments
Epidural neuroplasty stands out among other treatments for chronic spinal pain due to its targeted approach and minimal invasiveness. Unlike traditional spinal surgeries that require lengthy recovery periods, neuroplasty can provide rapid relief with far less risk.
In comparison to epidural steroid injections, which may require frequent repeat treatments, neuroplasty can offer longer-lasting results. While physical therapy and pain medications are common first-line treatments, they may not provide sufficient relief for all patients. Neuroplasty, however, targets the root cause of nerve compression, making it a more effective solution for many individuals.
Long-Term Outlook: Results and Follow-Up Care
The long-term results of epidural neuroplasty can vary, but many patients experience significant improvements in pain management and quality of life. Some individuals may need occasional follow-up procedures to maintain relief, especially if their underlying condition progresses.
To ensure the best possible long-term outcomes, patients are often advised to engage in lifestyle changes such as regular exercise, weight management, and ergonomic adjustments. Physical therapy may also be recommended to strengthen the muscles supporting the spine and prevent further damage.
With proper aftercare, including regular follow-up visits with the physician, many patients can enjoy years of pain-free or significantly reduced symptoms.
The Epidural Neuroplasty Procedure: What to Expect
On the day of the procedure, patients typically arrive at the outpatient facility and are prepared for the treatment. The process begins with a thorough consultation to review the patient’s medical history, followed by the administration of a local anesthetic to numb the skin and the area surrounding the spine.
Once the area is numbed, the doctor will insert a small needle or catheter into the epidural space, using fluoroscopy to guide the needle to the precise location of the nerve compression. This ensures the medication is delivered accurately and directly to the problem area. Once the catheter is in place, a combination of corticosteroids and local anesthetics is slowly injected to reduce inflammation and alleviate pain.
The procedure usually takes between 30 minutes to an hour, and patients are often able to go home the same day. Although some discomfort or mild soreness may be experienced in the first 24 hours, most patients are able to resume light activities within a few days.
Following the procedure, it’s recommended that patients avoid strenuous activities for a short period, and follow up with their doctor to track their recovery progress. Many patients experience significant pain relief immediately, but full results may take several days to become noticeable.
Future of Epidural Neuroplasty and Technological Advancements
The future of epidural neuroplasty looks promising, with ongoing advancements in medical technology making the procedure even more effective. New imaging techniques and refined catheter systems allow for even more precise targeting of nerve compression, improving patient outcomes.
Additionally, researchers are exploring the use of stem cell therapy and regenerative medicine in conjunction with neuroplasty to further enhance pain relief and accelerate recovery. As technology continues to evolve, epidural neuroplasty will likely become an even more integral part of pain management for individuals with chronic spinal conditions.
Recovery After Epidural Neuroplasty
The recovery process after epidural neuroplasty is generally quick, with most patients able to return home the same day. Immediately following the procedure, some mild soreness or discomfort at the injection site is common, but this usually subsides within 24 hours.
For the first few days, patients are encouraged to rest and avoid strenuous physical activity. However, walking and light stretching can help maintain mobility. Many individuals return to their normal activities within a few days, and most are able to resume work after a week, depending on the nature of their job.
Physical therapy may be recommended in some cases to help strengthen the muscles supporting the spine and improve long-term pain management. While the procedure offers immediate relief for many, full benefits can take several days to a few weeks to become apparent.
Frequently Asked Questions (FAQs) About Epidural Neuroplasty
1. Is epidural neuroplasty painful?
Most patients experience only mild discomfort during the procedure, thanks to local anesthesia used to numb the area. Afterward, some soreness or tenderness at the injection site may occur but typically subsides within a day.
2. How soon can I expect results?
While many patients report immediate relief, it can take several days to a week for full benefits to become noticeable. For some, the effects may last for months, depending on the individual’s condition.
3. Can epidural neuroplasty be repeated?
Yes, the procedure can be repeated if necessary, especially if pain recurs or the underlying condition progresses. However, the frequency of treatments is typically determined by the patient’s overall health and response to prior sessions.
4. Will insurance cover the procedure?
Coverage varies by insurance provider and policy, but many plans cover epidural neuroplasty when it is deemed medically necessary. It’s recommended to check with your insurance provider for specific details.
Conclusion
Minimally invasive epidural neuroplasty offers a safe, effective, and less invasive alternative to traditional spinal surgeries for patients suffering from chronic pain. By targeting the root cause of nerve compression, it provides lasting relief for many individuals with conditions like sciatica, radiculopathy, and spinal stenosis.
With its quick recovery times, minimal risk, and high success rates, epidural neuroplasty is quickly becoming a preferred option for people seeking pain relief without the need for extensive surgery. As technology continues to advance, the procedure’s effectiveness and precision will only improve, making it an increasingly attractive choice for chronic pain sufferers around the world.
For those exploring treatment options, it’s essential to consult with a skilled specialist who can help determine if epidural neuroplasty is the right solution for their specific condition.