Percutaneous Transhepatic Cholangiography
Overview
Noninvasive imaging might be difficult to evaluate patients with obstructive biliary pathology. Percutaneous cholangiopancreatography, in combination with endoscopic retrograde cholangiopancreatography, is essential for diagnosing and treating particular pathologies.
What is Percutaneous transhepatic cholangiography (PTC)?
Percutaneous transhepatic cholangiography (PTC) is a diagnostic and/or therapeutic treatment that involves first inserting a needle into the biliary tree and then inserting a catheter immediately thereafter (percutaneous biliary drainage or PBD). Contrast is injected into one or more bile ducts (cholangiography) and potentially the duodenum at some time during the operation. PTC can be done with either fluoroscopic or ultrasound (US) guidance.
Anatomy and Physiology
Understanding the intrahepatic and extrahepatic components of the biliary system is required for successful PC. The intrahepatic biliary ducts are part of the portal triad of the hepatic lobules, which also includes a biliary duct, hepatic artery, and portal vein. Until pathologically enlarged, they are often not visible in standard imaging investigations. The right and left hepatic ducts, common hepatic duct, cystic duct, gallbladder, and common bile duct are all extrahepatic biliary components. When doing cholangiography, it is critical to understand probable congenital defects. Abnormal biliary ducts, abnormal cystic duct insertion, choledochal cysts, diverticulum, and the anomalous junction of the biliary ductal and pancreatic ducts are all relevant defects.
Indications of PTC
Although PTC serves a diagnostic function, less invasive procedures to image the bile ducts and adjacent tissues should be considered first-line diagnostic procedures. These are some examples:
- US
- Computed tomography (CT)
- Magnetic resonance imaging (MRI) including cholangiopancreatography (MRCP)
- Endoscopic retrograde cholangiopancreatography (ERCP)
PTC is generally used for therapeutic objectives in cases of suspected or proven bile duct blockage, as well as to acquire diagnostic specimens, especially when ERCP is not a possibility or has been ineffective.
The disorders that impede bile drainage are classified into two types: malignant and benign. Malignant etiologies, notably cholangiocarcinoma, are more frequent in the United States. Bile duct stenosis is most commonly caused by benign disorders such as liver transplant-related stenoses and sclerosing cholangitis.
There are no medical society standards that give objective laboratory, symptom, or physical exam grades or cutoffs for grading the degree of biliary blockage in a systematic manner, or that address a standard for using PTC holistically with numerous algorithms. Some medical organizations, however, establish generic guidance in certain specific instances. There is an indication for intervention to alleviate the stricture in the setting of a suspected malignant stricture. The future hepatic remnant is the projected residual fraction of the liver (FLR). Any clogged ducts in the FLR should be emptied prior to hepatectomy in a person with a projected inadequately sized FLR.
According to the 2012 guidelines of the European Society of Gastrointestinal Endoscopy, preoperative drainage is only recommended for patients with potentially resectable malignant CBD obstruction who are candidates for neoadjuvant chemotherapy/radiation, have acute cholangitis, intense pruritus, and surgery can be delayed.
- The most frequent symptoms of bile duct blockage are nausea, anorexia, discomfort, and pruritis. Patients may appear with one or more of these symptoms. There are no objective criteria for determining how severe clinical symptoms should be before establishing PTC.
- PTC may be used to assist move bile away from the location of a biliary leak, such as after cholecystectomy.
- PTC is an alternate method of accessing the bile ducts in instances when ERCP is not possible (for example, post-Whipple surgery) or has failed, such as bile duct stone or bile duct stent extraction.
Sepsis caused by bile duct blockage is a sign of an effort to relieve the obstruction. Intravenous fluids and antibiotics should be administered initially. There are no evidence-based studies that indicate whether drainage should be undertaken immediately or after a short wait, such as 8 to 12 hours after antibiotics are started.
Some surgeons choose to treat bile duct blockage before doing a non-emergent or re-operation. In the case of unintentional CBD ligation, for example, the intrahepatic bile ducts can be emptied percutaneously prior to corrective surgery.
Contraindications
PC is contraindicated primarily when the risk of probable consequences is high or the likelihood of success is low. Several patient and illness characteristics influence the safety and success rate. The absolute contraindications for PC include irreversible coagulopathy or ongoing clopidogrel usage that cannot be stopped. Aspirin usage, big volume ascites, and hemodynamic instability are all relative contraindications. The majority of patients are critically ill, and clinicians should try to reverse any contraindications whenever possible.
Patient Preparation
In some cases, PTC should be avoided or postponed. As with any operations, it is best to begin with the least possibly damaging method of therapy. Correcting multisegmented obstructions with multiple areas of narrowing may not be advisable or even possible; instead, only the minimum required to provide a tolerable therapeutic result should be corrected. If the patient's survival is expected to be very short, the procedure should be reconsidered.
ERCP should be regarded as a potential first-line therapy for stenoses/obstructions that are accessible by this procedure, since it may avoid unwanted problems such as bleeding and the requirement for the implantation of a catheter that can only drain bile externally. ERCP is the first-line treatment for extrahepatic ductal lesions. There are currently no medical society recommendations for determining which patients should have ERCP first for intrahepatic ductal lesions.
Attempting PTC on a non-dilated ductal system, such as when the purpose is to redirect bile away from a CBD or cystic duct leak, dramatically increases the likelihood of failure. PTC can be briefly delayed if there is a probability that the ducts will expand with a short wait.
Certain considerations, such as the risks of bleeding and sedative issues, should be considered before undertaking the surgery, and such risks should be avoided if feasible. The Society of Interventional Radiology (SIR) presents a list of recommendations for the discontinuation of antiplatelet and anticoagulant drugs for interventional radiology procedures, which it categorizes from level 1 to level 3 based on bleeding concerns. PTC is classified as a category 2 procedure by the SIR. The SIR advises an INR of no more than 1.5 and a platelet count of at least 50,000 cells/microliter for such treatments.
How PTC is done?
PC is often performed in a radiology department with interventional capabilities. Image-guided percutaneous catheter placement requires additional training for interventional radiologists. Patients requiring PC typically have dilated bile ducts as a result of disease and blockages. This dilation makes it simpler to identify the biliary ducts on transabdominal ultrasonography or with any cross-sectional imaging modality, including magnetic resonance cholangiopancreatography and computed tomography.
Depending on the physician's discretion, there are several approaches to the biliary tree, including a mix of fluoroscopic and ultrasound-guided procedures. These imaging investigations are important and required for arranging all of the procedure's phases. PC may be technically restricted and linked with a greater frequency of problems if there is no visible dilation of the intrahepatic biliary channels.
- Patient's Position and Preparation
The patient should be in a supine posture that allows adequate access to the liver. The overlaying upper abdomen should be sterilely treated and draped. - Anesthesia
The surgery includes unpleasant measures such as a percutaneous catheter passing through the epidermis, intercostal muscles, and the liver capsule. As a result, the surgery should be carried out under local anaesthetic and mild sedation. Sedation is especially crucial when further procedures like as biopsies or stenting are required. - Antibiotic Prophylaxis
The obstructed biliary system requires Gram-negative bacteria and enterococcal antibiotic treatment.
What happens during a percutaneous transhepatic cholangiography?
- After your child has been given medicine to relax or sleep, the area above his abdomen is washed with a specific iodine solution and draped to avoid infection.
- His skin is injected with a local anesthetic (freezing drug). Once the region is numb, the interventional radiologist guides the needle into one of the bile ducts using ultrasound or x-ray pictures.
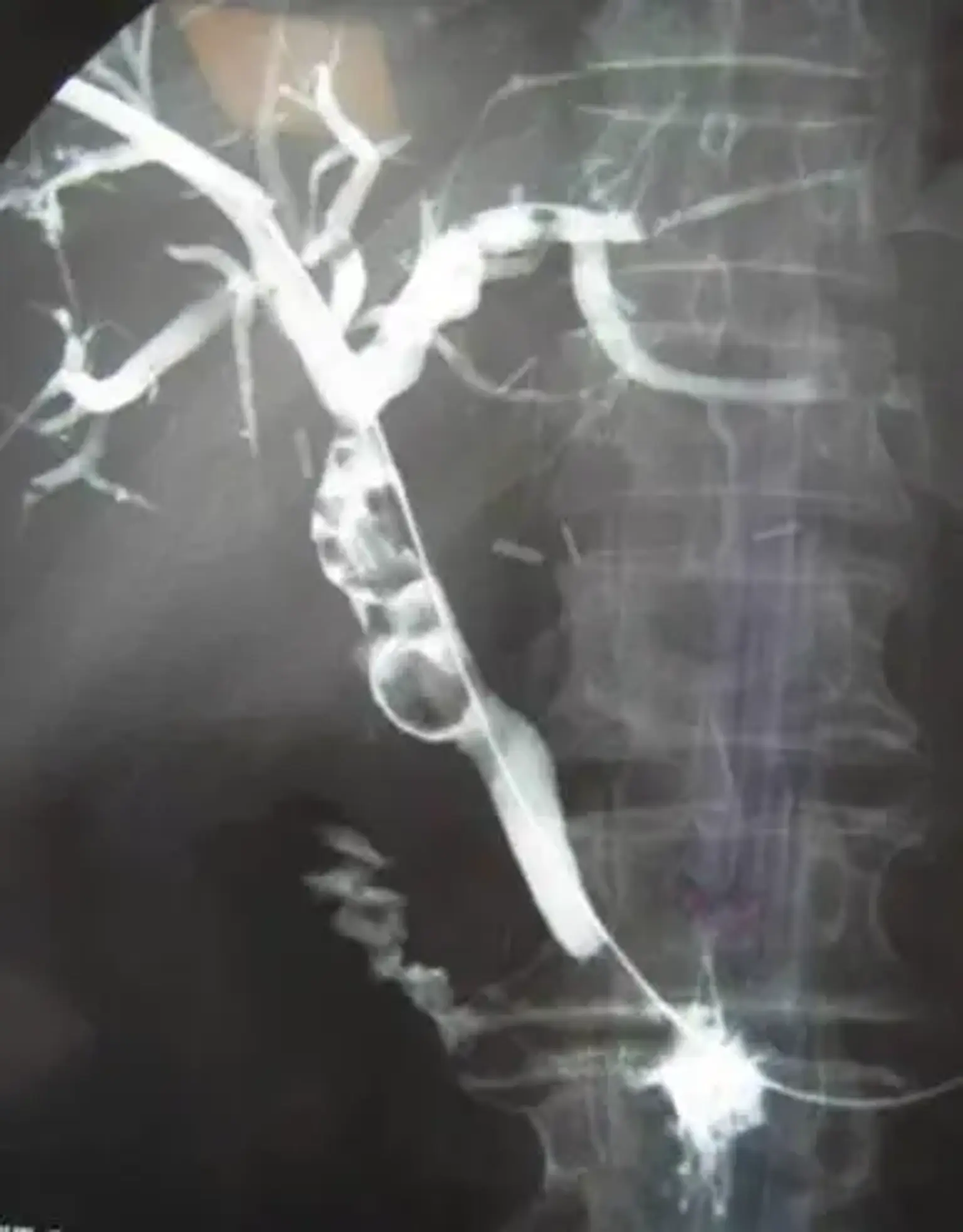
- The contrast medium is injected into the bile ducts once the needle is in a favorable location. The contrast injection enables the radiologist to examine all of the bile ducts in the liver and identify which are unusually obstructed or swollen. It also indicates the presence of any gallstones or other aberrant material within the bile ducts.
- To highlight all of the bile ducts, a series of x-ray pictures are acquired in various locations. To allow for more exact injection or to empty the bile, the radiologist may replace the needle with a tiny catheter (tube).
Three possible therapeutic options that can be performed through the catheter at the same time or during future procedures include:
- Balloon dilation of narrowing in the bile ducts
- Removal of gallstones with a special basket device
- Placement of a stent (tube of metallic mesh) across a blocked bile duct
Alternatively, the radiologist may decide to leave a special soft catheter in place to continue draining the bile.
What happens after the percutaneous transhepatic cholangiography?
- Your kid will be transported to the Interventional Radiology Post-Anesthesia Care Unit by a nurse (PACU). You will be permitted to visit the rehabilitation area.
- The nurse will closely observe your child until he is admitted or returns to his hospital bed.
- The interventional radiologist will discuss the procedure with you.
Is a percutaneous transhepatic cholangiography safe?
When conducted by a suitably qualified and experienced interventional radiologist, percutaneous transhepatic cholangiography is a safe technique that is generally performed under sedation or general anesthesia. Complications and adverse effects are possible with any invasive operation. These will be thoroughly explained to you before you give your consent.
During the process, your kid will be exposed to ionizing radiation (x-rays). We feel that the benefit to your child's health outweighs the risk of percutaneous transhepatic cholangiography. We have been leaders in adapting equipment and processes to provide the lowest feasible dosage to young patients since children are more vulnerable to radiation exposure than adults.
Complications
The incidence of serious problems for PTC and PBD is between 2% and 10%. Inducing sepsis, other serious infection (such as an abscess), bile leak/biloma, bleeding (subcapsular hematoma, pseudoaneurysm), pneumothorax, and death are all major consequences.
Blood vessel transgression is to be expected during PTC. Coagulation is normally effective, and the bleeding stops completely within 2 to 3 days. If a catheter side hole is left in communication with a hepatic vascular or a pseudoaneurysm develops, bleeding via the catheter may ensue.
- Hemodynamically Stable
If bleeding is visible (such as brilliant red pulsatile blood flowing out of the tube) in hemodynamically stable individuals, the patient should be brought for urgent angiographic embolization.
If bleeding is suspected, as evidenced by hemobilia, a dropping hemoglobin level, or unstable vital signs, CT angiography (CTA) is a first-line diagnostic technique. If evidence of bleeding is found on the CTA, digital subtraction angiography (DSA) through artery puncture can be done later for embolization therapy. When there is a high clinical suspicion of bleeding in the absence of hemorrhage on CTA, a fluoroscopic tractogram should be done next.
If no arteries are occluded or the drainage catheter sideholes are discovered to be outside the biliary tract, the catheter should be relocated and the tractogram repeated. An angiographic procedure with embolization should be explored. If a vein is opacified, the catheter should be enlarged to tamponade it. Time should be allowed to see if the intervention was effective. If an artery is occluded, the catheter should be enlarged to tamponade it. If blood may still be aspirated through the bigger catheter, angiographic embolization of the affected hepatic artery branch should be done as soon as possible.
- Hemodynamically Unstable
The radiologist and surgeon must agree on whether the patient should undergo surgery, angiography, or both if angiography can be performed in the operating room.
- Bleeding
- Tumor bleeding is possible, especially in hilar tumors. It is difficult to treat and may not respond to embolization or catheter implantation, necessitating surgery.
- Bleeding might occur after scheduled catheter removal in rare cases. In this case, the bleeding is virtually invariably venous and cannot be treated by angiography (i.e., arteriography). ERCP or a second PTC can be used to try to embolize the first tract.
Even little quantities of bile lining the skin, peritoneum, or pleura might produce considerable discomfort in some people, although a major leak may cause minimal pain in others. If bile seeps from the catheter or surrounding it into the abdomen (peritonitis) or chest (pleuritis), the catheter should be relocated, unclogged, and/or upsized to tamponade the leak. Biloma and/or subcapsular hematoma production does not require treatment in and of itself because the body may resorb the fluid; however, if the fluid becomes uncomfortable or infectious, it can be percutaneously drained.
If electrolyte depletion occurs as a result of high-output external drainage, the electrolytes should be replenished, and the catheter should be converted to internal drainage as soon as feasible.
PTC +/- PBD serves as a pathway for microorganisms to enter the biliary system from outside sources. Preventive methods include changing the catheter every 2 to 3 months and utilizing a catheter with a high possibility of remaining patent. Antibiotics are used to treat cholestasis.
Although PTC can be used to treat the blockage that is causing sepsis, it can also induce sepsis. In the setting of an intensive care unit, antibiotics, IV fluids, oxygen, and vasopressors should be considered.
- Catheter Dislodgement
Catheter dislodgement can occur even after the patient has been educated on how to avoid allowing traction to be applied on the catheter. Typically, a safety stitch at the skin's surface and/or a catheter with a self-retaining mechanism are employed. The first drainage catheter takes 4 to 6 weeks to create a stable patent tract, thus it is critical to take precautions to prevent catheter dislodgement during this period.
If the catheter has gotten partially dislodged, it may typically be simply reinstalled over a guidewire. If it has completely retreated from the liver, replacing it becomes considerably more difficult. If the catheter tract can be opacified with contrast, an angiographic type catheter and a guidewire can typically be utilized to navigate the transhepatic route before reinserting a new drainage catheter through the original tract.
Conclusion
Percutaneous cholangiography is an important tool for identifying and treating biliary disorders. ERCP and/or percutaneous cholangiography should be explored for patients who appear clinically with jaundice or symptoms of obstructive biliary disease, depending on the clinical presentation. Percutaneous cholangiography can help with the diagnosis and may guide future patient therapy.