Pulmonary Artery Catheterisation
Since Swan and Ganz and associates introduced pulmonary artery catheterization, there has been a lot of debate about its value. However, a study published by Connors and colleagues compared the consequences of critically ill patients treated with or without a pulmonary artery catheterization within the first 24 hours after admission to an intensive care unit and found a link between pulmonary artery catheterization and a steadily increasing relative risk of hospital mortality and resource utilization. This research renewed the debate and prompted physicians to reconsider the pulmonary artery catheterization efficacy and safety. Many studies demonstrate that pulmonary artery catheterization has almost no value or risk, while others demonstrate that it reduces death. Despite the controversies, doctors continue to utilize pulmonary artery catheterization in critically ill patients despite the lack of documented justifications.
Several hemodynamic measures are obtained using pulmonary artery catheterization. Heart rate, rhythms, cardiac output, pulmonary artery pressures, right atrial pressure (central venous pressure), pulmonary arterial occlusion pressure (wedge pressure), and mixed venous oxygen saturation are among the parameters that can be directly monitored. Many additional data, such as mean arterial pressure, body surface area, stroke volume, systemic and pulmonary vascular resistance, ventricular stroke workload, and oxygen supply and demand, can also be estimated using these variables.
A pulmonary artery catheter was originally intended to treat acute myocardial infarction, but it has since been used to treat a wide range of critical illnesses and surgical interventions.
What is a Pulmonary Artery Catheterization?
An intravascular catheter is put into a central vein (femoral, jugular, or brachial) to communicate to the right side of the heart and proceed towards the pulmonary artery during pulmonary artery catheterization. Right-sided cardiac compartment filling tensions, cardiac output estimates, intracardiac shunt assessment, valvular evaluations, and vascular resistance can all be assessed using this diagnostic method. Despite the decline in the use of pulmonary artery catheterization for the assessment and management of severely ill patients, it is still a valuable technique for evaluating patients with pulmonary hypertension, cardiogenic shock, and unexplainable breathlessness.
Anatomy and Physiology
The catheter is inserted into one of the main central veins (subclavian, jugular, or femoral) and travels to the right atrium through the superior or inferior vena cava. The catheter travels from the right atrium to the right ventricle via the tricuspid valve. After passing through the pulmonary valve, the catheter is moved to the right ventricular outflow tract and subsequently to the pulmonary artery. The catheters' tip is inserted into the major pulmonary artery, where the balloon can be expanded and released to take pressure readings. This is where a balloon can be inflated to obtain pulmonary capillary wedge pressure, which can be used to get an indirect reading of left-sided filling pressures.
A pressure waveform can be visible in the monitor during catheter insertion because of the transducer in the catheter. Each portion of the right heart structure has a different pattern that can aid in determining where the catheter points are located.
Pulmonary Artery Catheterization Indications
Pulmonary artery catheterization is suitable in the following cases:
- Acute coronary syndrome is expected
- Air emboli aspiration
- Coronary artery disease is expected
- On stress testing with imaging, high-risk results in symptomatic or asymptomatic individuals, or intermediate-risk results, discordant results, or equivocal/uninterpretable test results in symptomatic patients.
- On echocardiography, in the presence of recently identified, symptomatic left ventricular dysfunction; in the presence of symptomatic, new regional wall-motion abnormalities of unknown cause; or in the presence of suspected serious ischemic consequences due to coronary artery disease.
- For symptomatic stenosis of 50% or more on computed tomography angiography, left main or non-left main; for symptomatic stenosis of 50% or more in more than one coronary venous territory; for symptomatic lesions of unclear severity, potentially obstructive (non-left main); and for symptomatic or asymptomatic, potentially obstructive non-left main lesions.
Pulmonary Artery Catheterization Contraindications
In the following situations, pulmonary artery catheterization is not recommended:
- In the apparent lack of noninvasive stress imaging displaying occlusion of 50% or greater, coronary artery disease is suspected in an asymptomatic patient with low or intermediate global risk for coronary artery disease; when coronary artery disease is suspected in a symptomatic patient with low pretest possibility for coronary artery disease.
- In patients with a nonobstructive disease with obstruction of less than 50% who have unexpected angiographic findings or evidence of ischemia, or in the apparent lack of noninvasive testing, pulmonary artery catheterization is improper as adjunctive testing in patients receiving diagnostic coronary angiography.
- In patients at low risk for syncope, patients at low or intermediate risk for new-onset atrial fibrillation or flutter, and patients with heart block or symptomatic bradyarrhythmia, pulmonary artery catheterization is not recommended.
- Patients undergoing low-risk surgery, patients with 4 or more metabolic equivalents of functional capacity, patients with no risk factors who are to undergo intermediate-risk surgery or vascular surgery, and patients with one or two risk factors who are to undergo intermediate-risk surgery should not undergo pulmonary artery catheterization.
- Patients with mild or moderate mitral stenosis, mild or moderate mitral regurgitation, mild or moderate aortic stenosis, or mild or moderate aortic regurgitation should not undergo pulmonary artery catheterization.
- Pulmonary artery catheterization is unsuitable for the patients with chronic natural or artificial valve diseases who have symptoms related to their valvular disease, assuming that the patient's symptoms are consistent with the clinical impression of severity: Mitral stenosis; mitral regurgitation; aortic stenosis; and mild or moderate aortic regurgitation.
Equipment
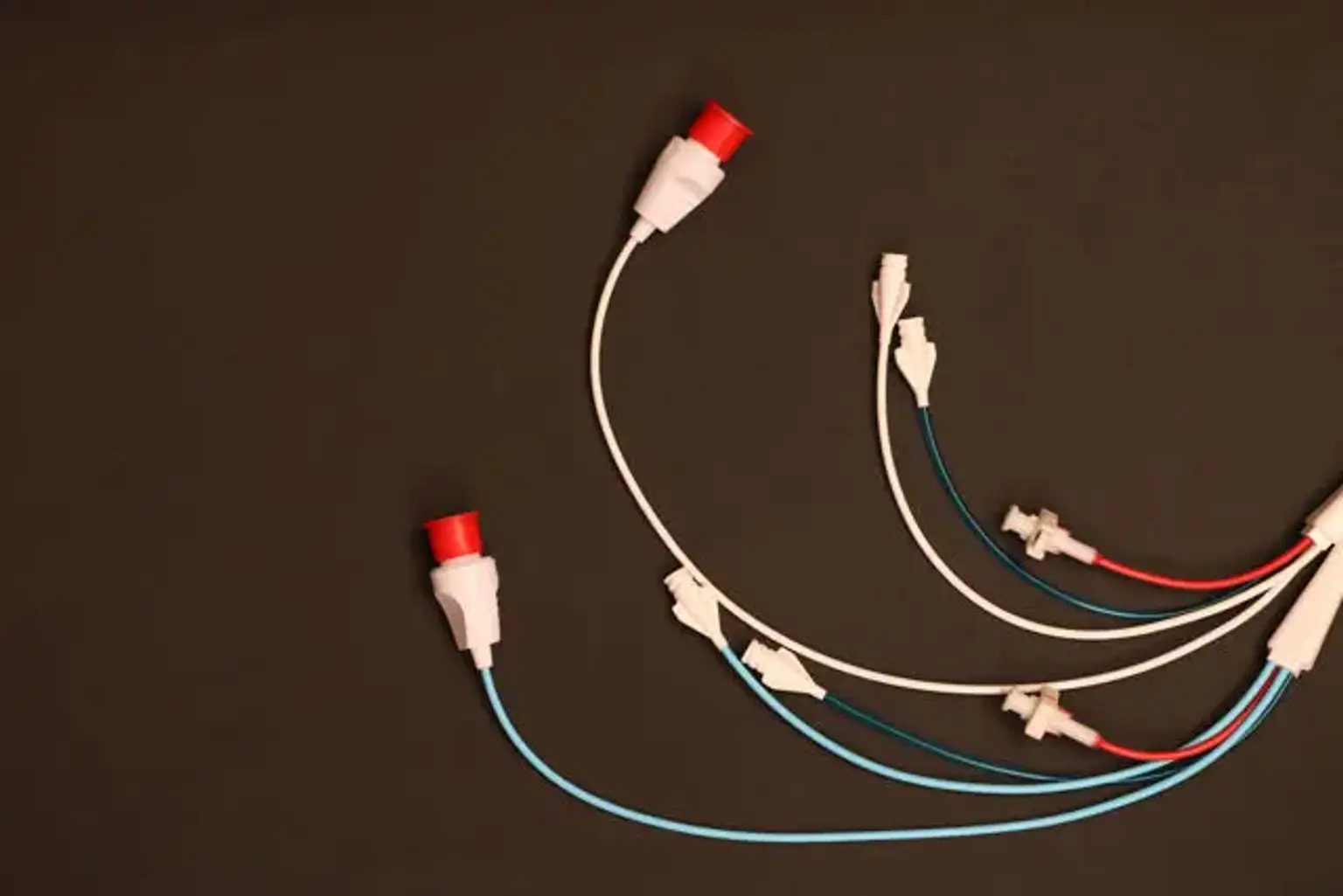
A Swan-Ganz catheter, also known as a right heart catheter, is a lumen catheter with a thermodilution sensor connected to an external pressure transducer. With this transducer, the central venous pressure, right atrial pressure, right ventricular pressure, and pulmonary artery pressure can all be determined.
Each of the four lumens is spaced at a specified distance along the catheters' length, and each has a distinct role, as stated below:
- The right atrial lumen is represented by the blue lumen or central venous pressure port. It is about 30 cm from the catheters' tip and is positioned inside the right atrium. It's the closest port to the heart and can be utilized for infusions. The central venous pressure and right atrial pressure can be measured via this port.
- The white lumen ends in the right atrium, adjacent to the previous lumen, at approximately 31 cm from the tip of the catheter. Infusions are administered through this port.
- The pulmonary artery lumen, also known as pulmonary artery distal, is the distal port at the catheter's tip. The pulmonary artery pressure is measured using this port. This port can also be used to draw mixed venous.
- The thermistor is a red/white connector with a temperature-sensitive wire that ends four centimeters from the catheter tip. The thermistor bead, which sits in a main pulmonary artery when the catheter tip is properly placed, is the terminal part of the wire. Thermodilution can be used to determine a cardiac output when the thermistor port is connected to a cardiac output monitor.
The balloon port is the red port. When the balloon requires to be collapsed, the air is injected and withdrawn. A balloon on the pulmonary artery catheter can be expanded to assist the doctor in placing the catheter tip in the pulmonary artery. There are black markings inside the catheter that can be used to measure the length of the catheter.
Preparation
The preparation for the insertion of a pulmonary artery catheter is comparable to that for any other invasive surgery.
Before the procedure, you must give your verbal approval. Before beginning the process, a thorough description of the procedure, its risks, and its advantages is required.
Before beginning the procedure, the catheterization site must be chosen. To avoid difficulties, extra care must be given while choosing the insertion location, such as skin or site infections, previous vein thrombosis, or anatomical anomalies. It is critical to choose the right catheter for the insertion site.
During the procedure, sterile barriers and methods must be used. Cleansing the insertion site and covering the patient are both required. Additionally, the individual performing the procedure must wear personal protective equipment and a sterile barrier such as sterile gloves, a mask, and a surgical gown.
Pulmonary artery catheterization can be performed under fluoroscopy (the most frequent method) or at the bedside using ultrasonography and echocardiography.
Equipment Setup
Zero References
Any motion of the transducer or the patient will modify the hydrostatic column of this fluid-filled system, causing the pressure readings to change. The system must therefore be reset to ambient air pressure before or after pulmonary artery catheter insertion.
The center of the left atrium, considered as the fourth intercostal space in the midaxillary line with the patient in the supine position, serves as a reference point. The membrane is subjected to air pressure with the transducer at this level, and the monitor is reset to zero.
Calibration
The monitoring system must be adjusted for accuracy after it has been zeroed. Presently, most monitors undergo an electronic calibration that is automatic.
The system is manually calibrated and checked using the following two methods:
- The distal tip of the pulmonary artery catheter is elevated to a specified height above the left atrium if the catheter has not been placed. If the apparatus is functioning perfectly, lifting the tip 20 cm above the left atrium should result in a measurement of roughly 15 mm Hg.
- Furthermore, using mercury or aneroid manometer, pressure can be delivered outside to the transducer and calibrated to a predetermined level. The system is then calibrated when the monitor is set to read this pressure.
Dynamic Tuning
Central pressures have a periodic frequency because they are dynamic waveforms. The system needs the right frequency response to properly monitor these pressures. When a system is slow to respond, pressure measures are imprecise, and differentiating waveforms becomes challenging. The pressure waveform is attenuated when signal energy is lost. Air bubbles, lengthy or compliant tubing, vessel wall impingement, intra-catheter material, transducer dysfunction, and loose tubing interconnections are some of the most common reasons. The frequency response is tested qualitatively by flicking the catheter and looking for a vigorous high-frequency response in the waveform.
The rapid flush test can be used to check the system after it has been inserted. A suitably responsive system will display an initial horizontal line with a high-pressure reading when flushed. When the flushing is finished, the pressure reduces quickly, as shown by a vertical line that drops below the baseline. Following a brief and well-defined oscillation, the pulmonary artery waveform returns. A dampened system won't overrun or oscillate, but it will take longer to go back to the pulmonary artery waveform.
Pulmonary Artery Catheterization Procedure
Using the modified Seldinger technique, implant the introducer sheath. Use the needle to inject lidocaine into the skin and subcutaneous tissue. Then, while providing negative pressure to the syringe, insert the needle into the vein. Ultrasound can be used to see where the needle is entering the body.
Withdraw the syringe and place the guidewire into the needle once dark-red, non-pulsatile blood has been aspirated. Stabbing the skin close to the needle with the scalpel, then removing the needle. Place the sheath and internal obturator over the guidewire until the hub occupies the wound while maintaining the guidewire to ensure that it stays open and does not embolize. To guarantee rapid flow, detach the obturator and guidewire from the sheath and connect a sterile flush to the port.
Connect the pulmonary-artery catheter's distal port to the main pressure monitor. Lower the pressure to zero and put the catheter tip level with the patient's heart. Place the catheter into the sheath after orienting it such that its curve follows the intended course. Pump up the balloon after advancing the catheter to halfway between the first two thin marks, at which point its tip will be outside the sheath.
Continue advancing the catheter until you see a right-atrial-pressure waveform. An internal jugular or subclavian vein is normally 14 to 20 cm away from the right atrium, while a femoral vein is often 37 to 50 cm away. An a wave implies atrial contraction; an x descent implies atrial relaxation; a small c wave implies tricuspid valve closure; a v wave implies passive atrial filling during right ventricular systole; and a y descent implies passive atrial unloading following the opening of the tricuspid valve are all recognizable components of the right atrial waveform. Make a note of the mean right atrial pressure with the help of an assistant.
Transduce a right-ventricular-pressure waveform by advancing the catheter another 4 to 10 cm. This sinusoidal waveform has a fast upstroke and downstroke, which depict ventricular systole, as well as a delayed upstroke, which represents passive ventricular filling during diastole followed by right atrial contraction. Instruct an assistant to record the systolic and diastolic pressures in the right ventricle.
Transduce a pulmonary-artery-pressure waveform by advancing the catheter another 4 to 10 cm. This waveform has a systolic-pressure waveform as well, but it differs from the right ventricular waveform by a gradual drop in pressure throughout diastole rather than an increase, an overall increase in diastolic pressure, and a dicrotic notch. Tell the assistant to record the pulmonary-artery pressures in systolic, diastolic, and mean.
When the waveform showing pulmonary-capillary wedge pressure is transduced, move the catheter. This waveform is identical to the right atrial waveform, but during respiration, there may be more fluctuation. Whether the patient is breathing naturally or receiving mechanical ventilation, tell your assistant to record the mean pressure at the end of expiration. Although positive end-expiratory pressure can impact pulmonary-capillary wedge pressure readings, the effect is usually insignificant when pulmonary-capillary wedge pressure is less than 10 cm of water.
Deflate the balloon when all measurements have been finished and check for the return of a pulmonary-artery-pressure waveform. If the waveform does not occur after a few moments, carefully pull the catheter until it does.
To determine the mixed venous oxygen saturation, aspirate blood from the distal port. Attach the thermistor to a computer and deliver a saline bolus into the right atrium through the proximal port to measure the cardiac output. The area under the curve is inversely associated with cardiac output. Calculate the average of the data after repeating the cardiac output test till at least three reliable values have been recorded.
Take note of the catheters' final position. Check to see if the balloon has deflated. Secure the catheter with the plastic sleeve attached to the sheath, which may lower the risk of infection. Use adhesive dressing after suturing the sheath to the skin.
Pulmonary Artery Catheterization Complications
The initial venous entrance, insertion of the pulmonary artery catheter, and maintaining the catheter within the pulmonary artery are all related to pulmonary artery catheterization complications. The risk of complications varies depending on the doctor's level of experience and the patient's condition. Even when using ultrasonography-guided methods, venous access complications can occur, such as arterial rupture, which can manifest instantly (e.g., carotid artery hematoma if placed via the internal jugular path) or insidiously (eg, hemothorax if placed via subclavian path). Pneumothorax risk is also related to the access route chosen, with pneumothorax happening more frequently in the subclavian than at the internal jugular site. However, it's worth noting that low internal jugular approaches also carry danger. Remember that tension pneumothorax can develop quickly in ventilated patients.
The most prevalent consequence linked with pulmonary artery catheterization placement is arrhythmias. Premature ventricular contractions or non-sustained ventricular tachycardia are the most common, and they can be treated by moving the catheter from the right ventricle to the pulmonary artery or quickly withdrawing it from the right atrium. Only around 1% of patients experience significant ventricular tachycardia or ventricular fibrillation that requires therapy, usually in conjunction with cardiac ischemia or electrolyte abnormalities.
Right bundle-branch block can happen after pulmonary artery catheterization placement and is usually temporary once the catheter is positioned in the pulmonary artery. However, if the patient has a previous left bundle-branch block, right bundle-branch block puts them at risk for complete heart block. Temporary pacemaker devices should be kept on hand for these individuals. The pulmonary artery catheterization cinching on itself or intracardiac structures is quite uncommon. This danger may be enhanced in patients with dilated heart chambers or in cases where the right ventricle tracing persists despite the pulmonary artery catheterization being advanced further 20 cm.
Pulmonary artery rupture is the most dangerous of the problems associated with pulmonary artery catheterization maintenance, with a 50% fatality rate. Thankfully, it's a rare event. Patients with pulmonary hypertension, those over the age of 60, and those on anticoagulant therapy are at threat. This scenario is indicated by the quick onset of hemoptysis. Higher positive end-expiratory pressure, lateral decubitus position, intubation with a double-lumen endotracheal tube comprise the proper management for this condition. If bleeding persists or becomes significant, bronchoscopy, angiography, or lobectomy may be required. The use of a vascular plug to compress the culprit pulmonary artery leak is described in a case report.
Infection caused by pulmonary artery catheterization is a pretty common consequence. In other studies, the rate of positive catheter tip culture results is as high as 45 percent. Although sterile plastic sleeves have been utilized to reduce the infection risk with pulmonary artery catheterizations, a prospective observational study discovered positive cultures from the sleeve in some patients, so the sleeve should not be regarded as a sterile barrier. Thankfully, the chance of developing clinical sepsis is less than 0.5 percent per day spent with a catheter.
After 4 days of catheterization, the risk of severe catheter colonization doubles. To avoid catheter-related infection, the US Centers for Disease Control and Prevention advises against replacing pulmonary artery catheterization on a regular basis.
Pulmonary infarction is a rare occurrence. The most common cause is an unintentional distal displacement of the pulmonary artery catheter tip. Catheter-related thrombi may also be a substantial cause. While postmortem investigations have demonstrated a considerable increase in endocardial lesions (e.g., thrombi, hemorrhage, and vegetations) associated with pulmonary artery catheter usage, no link to clinical outcomes has been identified.
Conclusion
Pulmonary artery catheterization can be conducted securely at the patient's bedside and provides a wealth of hemodynamic parameters. Although current research suggests that this procedure should not be used frequently in critically ill patients, it is still useful in the detection and treatment of a variety of cardiovascular diseases. However, because the operation has the potential for deadly consequences, it should only be used when the results are likely to improve clinical care.