Radiofrequency ablation
Overview
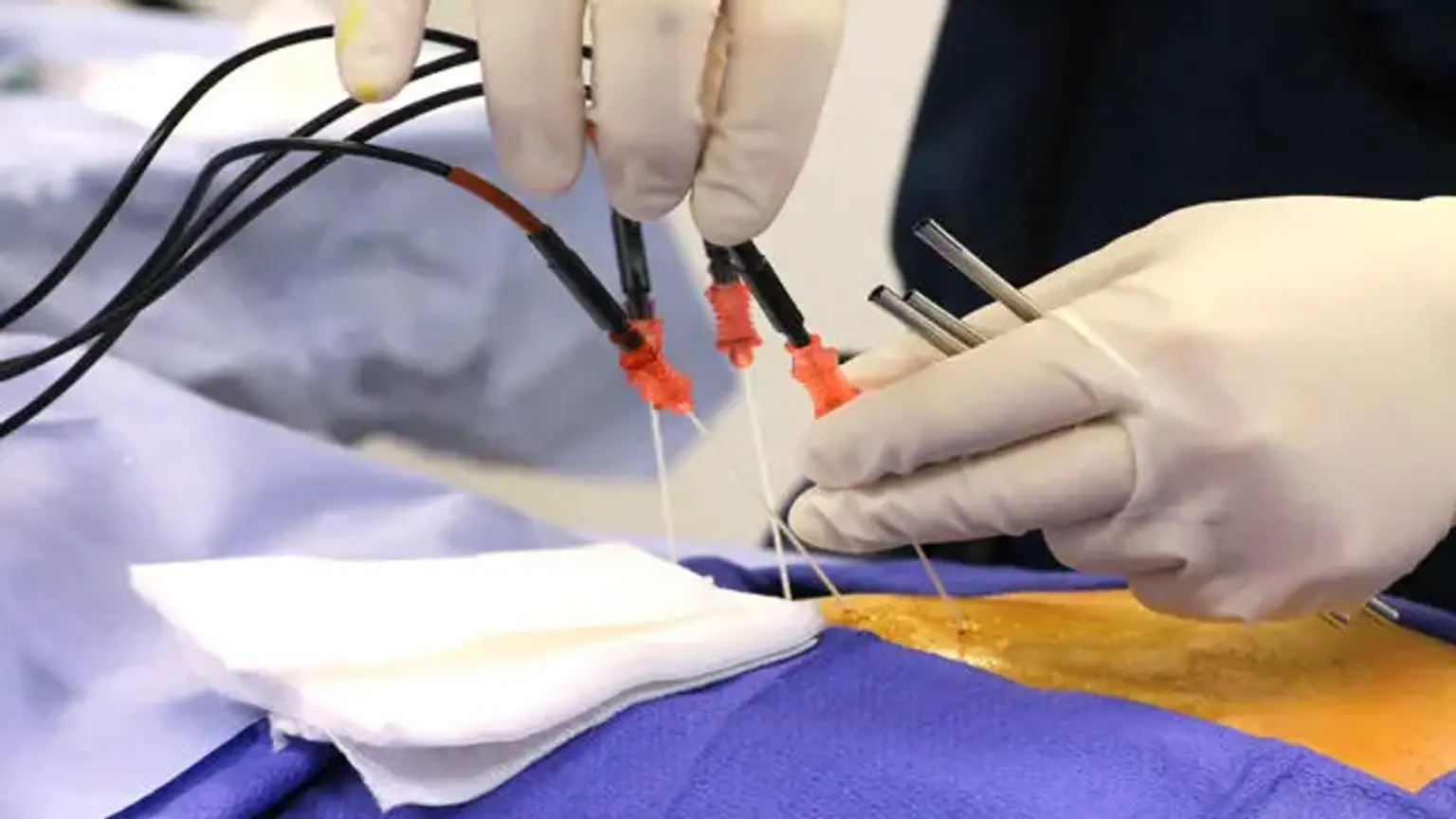
Radiofrequency ablation involves the use of an electric current to burn up a tiny region of nerve tissue in order to prevent it from delivering pain signals. It can give long-term relief for patients suffering from chronic pain, particularly in the lower back, neck, and arthritic joints.
The use of radiofrequency ablation for chronic pain is based on the assumption that passing radiofrequency currents near nociceptive pathways may disrupt pain signals. The heat energy linked with radiofrequency ablation causes tissue damage, with the nerves responsible for transmitting and/or modifying pain sensations being targeted.
Radiofrequency ablation definition
Radiofrequency ablation (RFA), also known as fulguration, is a medical technique in which a portion of the electrical conduction system of the heart, tumor, or other defective tissue is ablated using heat generated by medium frequency alternating current .
Electrical currents have been used to induce predictable thermal lesions since the 1950s; however, the use of radiofrequency for chronic pain did not emerge in the literature until the 1970s. The basic assumption is that radiofrequency currents are supplied through an electrode positioned near a nociceptive pathway to disrupt pain signals.
Thermal energy causes a predictable region of tissue death that is aimed at containing the nerves responsible for transmitting and/or regulating pain feeling. Today, there are several types of thermal ablative methods based on the previously described basic assumption.
Anatomy and Physiology
Thermal energy is commonly used to treat chronic back and neck pain disorders by applying it near or on the peripheral nerve sources along the levels of the spinal cord. It has been used to treat facet joint discomfort by focusing on the medial branch of the major dorsal ramus. It has also been used to treat discogenic back pain by targeting the ramus communicans.
The dorsal root ganglia is another target for radicular back pain, and the lateral branch neve is another for sacroiliac illness. The research also shows effectiveness in face pain syndromes, thoracic pain, and anterior/posterior pelvic pain syndromes on a less frequent basis.
Indications
Lesions formed at 40 and 67 degrees Celsius have little clinical relevance. The authors speculated that the therapeutic advantages may be attributed to electrical currents rather than temperature. This resulted in the invention of pulsed radiofrequency (PRF). They hypothesized that by applying higher voltage radiofrequency currents in a pulsatile way, they may avoid neurodestructive temperatures, giving the heat time to disperse and reducing the danger of thermal tissue harm.
Following PRF administration, lab investigations revealed signs of brain stress and cellular substructure damage. Later research, however, demonstrated that the poor reaction time of temperature-measuring instruments could not reliably exclude the possibility of transient temperature spikes, undermining the function of electrical currents in producing tissue harm.
There is currently no clear evidence of pain pathway impairment in response to high-frequency electrical current. It is believed that the therapeutic advantages reported are the result of a combined involvement of electrical and thermal damage. PRF has risen in popularity and utility above conventional radiofrequency ablation due to its perceived safety and therapeutic effectiveness.
PRF has been utilized to treat the dorsal root ganglion at all levels of the spine in a variety of pain syndromes, including radicular pain, discogenic pain, facetogenic pain, post-herpetic neuralgia, post-amputation pain, and post-inguinal herniorrhaphy pain. It can also be used in conjunction with other peripheral nerves, such as the medial branch nerve, suprascapular nerve, intercostal nerve, and pudendal nerve.
This enables for the treatment of a wide range of diseases, from shoulder pain to meralgia paresthetica. The splanchnic nerves are used for pancreatic discomfort, while the dorsal penile nerves are used for premature ejaculation. It also affects the central nervous system and autonomic ganglia in the case of trigeminal neuralgia, the sphenopalatine ganglion in the case of head and neck pain, and the lumbar sympathetic chain in the case of complicated regional pain syndrome.
Water-cooled radiofrequency (WCRF) ablation is another type of radiofrequency ablation. Previous approaches in cardiac electrophysiology and tumor ablation were used to develop this technique. While the idea remains substantially the same, WCRF uses a continuous flow of water to cool a multichannel electrode.
This active cooling method keeps the electrode from reaching excessive tissue temperatures. As a result, the RF current might continue to flow indefinitely, causing a greater thermal lesion. Furthermore, the WCRF lesion produces a distinct lesion with a substantially colder immediate spherical region, known as an isotherm, around the probe. Following that, there is a hotter isotherm, with successively lower temperature isotherms following as the distance from the probe increases.
Lesion size, like that of traditional radiofrequency ablation, is affected by probe size, electrode temperature, and current duration. Active and passive heat sinks are two more elements that might influence the size and appearance of the lesion. Blood flow in the epidural venous plexus and cerebrospinal fluid flow in the thecal sac are both active heat sinks. Muscular and boney structures are examples of passive heat sinks.
Cryoneurolysis is an alternate approach in the field of thermal neurolytic treatment. The advantages of this method include the absence of neuroma development or hyperalgesia, which can be side effects of surgical sectioning, radiofrequency ablation, or chemical neurolysis. The process of cryoneurolysis appears to be caused by injury to the vasa nervorum, which causes endoneurial edema, pressure, and axonal death.
Nerves regenerate at a pace of approximately 1 to 1.5 millimeters per week from preserved connective tissue components and Schwann cell basal lamina. The time it takes for proximal axons to reinnervate their targeted tissues determines the duration of analgesia, which normally spans from weeks to months. The most common application of cryoneurolysis mentioned in the literature is for the management of post-thoracotomy pain.
This success led to its use in various chronic pain syndromes, such as trigeminal neuralgia, atypical facial pain, spinal and extremities aches, abdominal pain syndromes, and atypical perineal pain. The proceduralist's experience appears to be the sole restriction to the range of cryoablation's utility.
Tumors treated with RFA
RFA can be used to treat malignancies in the lung, liver, kidney, and bone, as well as less often in other bodily organs. Once the tumor's diagnosis is confirmed, a needle-like RFA probe is inserted into the tumor. The radiofrequency waves traveling via the probe raise the temperature within tumor tissue, resulting in tumor elimination. RFA can be used to treat tiny cancers, whether they originated within the organ (primary tumors) or spread to the organ (secondary tumors) (metastases). The appropriateness of RFA for a certain tumor is determined by a number of criteria.
RFA is normally performed as an outpatient operation, however, it may occasionally necessitate a brief hospital stay. To treat hepatocellular carcinoma, RFA may be coupled with locally administered chemotherapy (primary liver cancer). As a therapy for hepatocellular carcinoma, a technique now in phase III trials employs the RFA probe's low-level heat (hyperthermia) to stimulate the release of concentrated chemotherapeutic medicines from heat-sensitive liposomes in the margins around the ablated tissue (HCC). Radiofrequency ablation is also employed in the treatment of pancreatic and bile duct cancer.
RFA has grown in importance in the treatment of benign bone tumors, most notably osteoid osteomas. Since its introduction in the 1990s for the treatment of osteoid osteomas, the procedure has been shown in numerous studies to be less invasive and expensive, to result in less bone destruction, and to have comparable safety and efficacy to surgical techniques, with 66 to 95 percent of people reporting symptom relief.
While RFA has a high initial success rate, symptom recurrence following RFA therapy has been recorded, with some studies revealing a recurrence rate comparable to surgical treatment. RFA is also being utilized more often in the palliative treatment of painful metastatic bone disease in patients who are ineligible for or do not respond to standard treatments
Radiofrequency energy for heart diseases
Radiofrequency radiation is utilized to remove aberrant electrical pathways that contribute to cardiac arrhythmias in heart tissue or normal portions. It is used to treat recurrent atrial flutter (Afl), atrial fibrillation (AF), supraventricular tachycardia (SVT), atrial tachycardia, Multifocal Atrial Tachycardia (MAT), and certain ventricular arrhythmias. The energy-emitting probe (electrode) is attached to the tip of a catheter, which is inserted into the heart via a vein. This catheter is known as an ablator.
Before removing the responsible tissue, the practitioner "maps" a region of the heart to find the aberrant electrical activity (electrophysiology research). Ablation is currently the conventional treatment for SVT and normal atrial flutter, and it can also be used in AF, either to block the atrioventricular node after pacemaker placement or to disrupt conduction inside the left atrium, particularly around the pulmonary veins.
In some cases, such as forms of intra-nodal re-entry (the most common type of SVT), also known as atrioventricular nodal reentrant tachycardia or AVNRT, ablation can be accomplished through cryoablation (tissue freezing using a coolant that flows through the catheter), which avoids the risk of complete heart block, which can be a complication of radiofrequency ablation in this condition.
Cryoablation, on the other hand, has a greater recurrence rate. Microwave ablation, in which tissue is ablated by the microwave energy "frying" the nearby tissue, ultrasonic ablation, in which mechanical vibration creates a heating effect, and laser ablation have also been created but are not widely used.
Contraindications
Radiofrequency ablation has just a few contraindications. Patient refusal, elevated intracranial pressure, and local infection are all absolute contraindications. Because numerous operations are performed close to the spinal column, strong clinical judgment and standard of care must be used when dealing with anticoagulant drugs and bleeding diathesis.
Coagulation studies should be revisited as needed. Bacteremia and abnormal congenital or surgical anatomy are relative contraindications. Because these are elective operations, it is critical to consider the risks and benefits, as well as document patient agreement and comprehension.
The procedure
Equipment
As with many operations, appropriate room to support necessary material and employees is required from the outset. A procedure table/bed that will comfortably support the patient while limiting positioning harm, fluoroscopic imaging equipment, and a table to lay surgical tools sterilely are among the larger components.
Monitors should be utilized to check the patient's oxygenation, breathing, circulation, and temperature, especially if sedation is being considered. A qualified anesthesia professional must also be present if deep sedation or general anesthesia is necessary. Introducer needles, catheters with electrodes, and an equipment interface are utilized during the process. Supplemental oxygen, suction, and a code cart should be nearby and easily accessible.
Personnel
Thermal nerve ablative methods should only be used by highly experienced professionals who have prior expertise doing spinal surgeries under fluoroscopy. These are often board-certified, fellowship-trained pain medicine specialists with backgrounds in anesthesiology, physical medicine and rehabilitation (PM&R), family medicine, neurology, emergency medicine, and psychiatry.
A circulating nurse is often present to assist with equipment and patient support, as is the case with many other operations. A radiology technician also aids with radiographic imaging.
Technique
To inhibit pain signals, catheter-guided radiofrequency currents are delivered through an electrode positioned near a nociceptive route. This is done with the use of a fluoroscope. Surprisingly, the currents heat the tissue around the electrode while the electrode itself is passively heated by the surrounding tissue.
When the target temperature is attained, the current is turned off in a standard radiofrequency procedure. The current is then turned on to keep the tissue temperature at a specified level.
The cycling of on-and-off currents keeps the specified tissue temperature constant. Nerve tissue begins to be damaged at temperatures over 45 degrees Celsius; however, care must be taken not to elevate temperatures above the point of tissue gas production (80 to 90 degrees Celsius). While early research showed that unmyelinated C- and A-delta fibers were selectively destroyed at particular temperatures, further data demonstrated that all nerve fibers were destroyed undifferentially after radiofrequency treatment.
High-temperature radiofrequency ablation has typically been confined to facet denervation to minimize thermal harm to sensory and motor fibers; nevertheless, an arbitrary range of 55 to 70 degrees Celsius is employed for dorsal root ganglion lesioning. Radiofrequency currents are cycled for 20 milliseconds at 2 Hz for 120 seconds during PRF. The voltage is set so that the maximum temperature stays below 42 degrees Celsius.
Currently, the use of water-cooled radiofrequency (WCRF) is restricted to clinical presentations in which the pain generator is thought to have many innervation sources. WCRF has two fundamental approaches. For sacroiliac joint dysfunction, the monopolar approach is employed, while for discogenic pain, the bipolar technique is used. A 17-gauge electrode with a 4-millimeter active tip was utilized to apply 150 seconds of current with a temperature target of 60 degrees Celsius for sacroiliac joint dysfunction.
Cooling procedures have been known to promote analgesia since ancient times; nevertheless, a threshold temperature of -20 degrees Celsius must be attained to achieve long-term neurolytic effects. Furthermore, the effectiveness is affected not only by temperature, but also by the duration of cryosectioning, probe size, probe closeness to the target nerve, and the number of freeze cycles used. The contemporary cryoprobe is a double-lumen aluminum tube that connects to a carbon dioxide or nitrous oxide gas source. Typically, the probe temperature goal ranges between -50 and -70 degrees Celsius.
Complications
Bleeding, infection, needle insertion-induced nerve injury, placement, and burns produced by poor grounding pad placement are all potential side effects of thermal lesioning. The most prevalent problem is post-procedural soreness, which is, thankfully, temporary. Although there is a lesser likelihood of neuroma development and nerve regeneration following cryoneurolysis, neuropathic pain is the most commonly reported consequence.
Alopecia and pigmentation abnormalities have also been recorded, which is especially problematic when thermal lesions are done close to the face. Fortunately, side effects and problems from thermal neurolytic treatment are quite uncommon. Proper technique, radiographic guidance, sterile procedure, suitable pre-procedural checklists, and greater procedural expertise can reduce risk and incidence.
Clinical Significance
Examining the clinical effectiveness of various treatment methods can aid in the development of a successful technique. The most common application of pulsed radiofrequency has been for the treatment of cervical or lumbar radicular pain. PRF has also been demonstrated to be effective in the treatment of facet syndrome.
PRF has been shown to be clinically effective in the treatment of trigeminal neuralgia, and several case studies have described its usage for shoulder pain. Other PRF solutions have relied on single case reports or case series. Despite the fact that observational studies suggest its usefulness, bigger controlled trials are required because present data reveal varying efficacy for diverse reported illnesses. Furthermore, the stated efficacy was mostly short-term.
One 15-patient case series indicated clinical effectiveness for water-cooled radiofrequency ablation (WCRF) in patients with discogenic pain. Other case reports back up its use and demonstrate how clinical efficacy is still in its early stages. As previously noted, the majority of cryoablation's recorded usage is in post-thoracotomy pain, with much data dating back to the 1980s.
The approach was used due to an increased prevalence of neuropathic pain in the research group. There have been several reports of cryoablation for discomfort in the head, face, and neck.
The use of cryoablation in postoperative pain following herniorrhaphy decreased the research group's use of postoperative analgesics. The other two trials found no statistically significant differences in analgesic usage or pain ratings, but they did find an increased incidence of sensory disturbances in the treatment arm.
Chronic pain remains one of the most difficult disorders to manage. As a result of its multifactorial character, therapy is multimodal, encompassing medicinal, physical, and interventional treatments. As the medical community battles to limit the use of narcotics in the treatment of chronic pain, the use of interventional procedures will remain important therapy choice in the fight against intractable pain. Radiofrequency ablation, when done correctly, has clinically helped in symptomatic alleviation and reduced pharmaceutical reliance in this complex diagnosis.
Conclusion
Radiofrequency ablation is commonly used to treat pain and a variety of other illnesses. It should be noted that this approach is only one form of pain control, and it has its drawbacks. It is not a replacement for other forms of pain relief, but rather a complimentary therapy. An interprofessional approach including nurses and pharmacists may aid in the selection of patients most likely to benefit from this treatment. Once chosen, the technique needs interprofessional collaboration to be successful.
Typically, the surgeon, an ultrasound technician, and a nurse are involved. The ultrasound technician will help with positioning and confirmation. Because the patient is normally awake during the surgery, the nurse will aid in monitoring vital signs and alleviating anxiety. Any widely used drugs should be available to the nurse. The interprofessional team must be aware of and prepared to deal with any issues that may arise.
Furthermore, members of the team must quickly disclose any concerns to the operational surgeon doing the procedure. Nursing supervision will be maintained following therapy. Furthermore, patient education is frequently required, with concerns of the patient that the nurse cannot address being conveyed to the surgeon for further discussion. An interprofessional team approach yields the greatest results with radiofrequency ablation.