Robot Colectomy
Overview
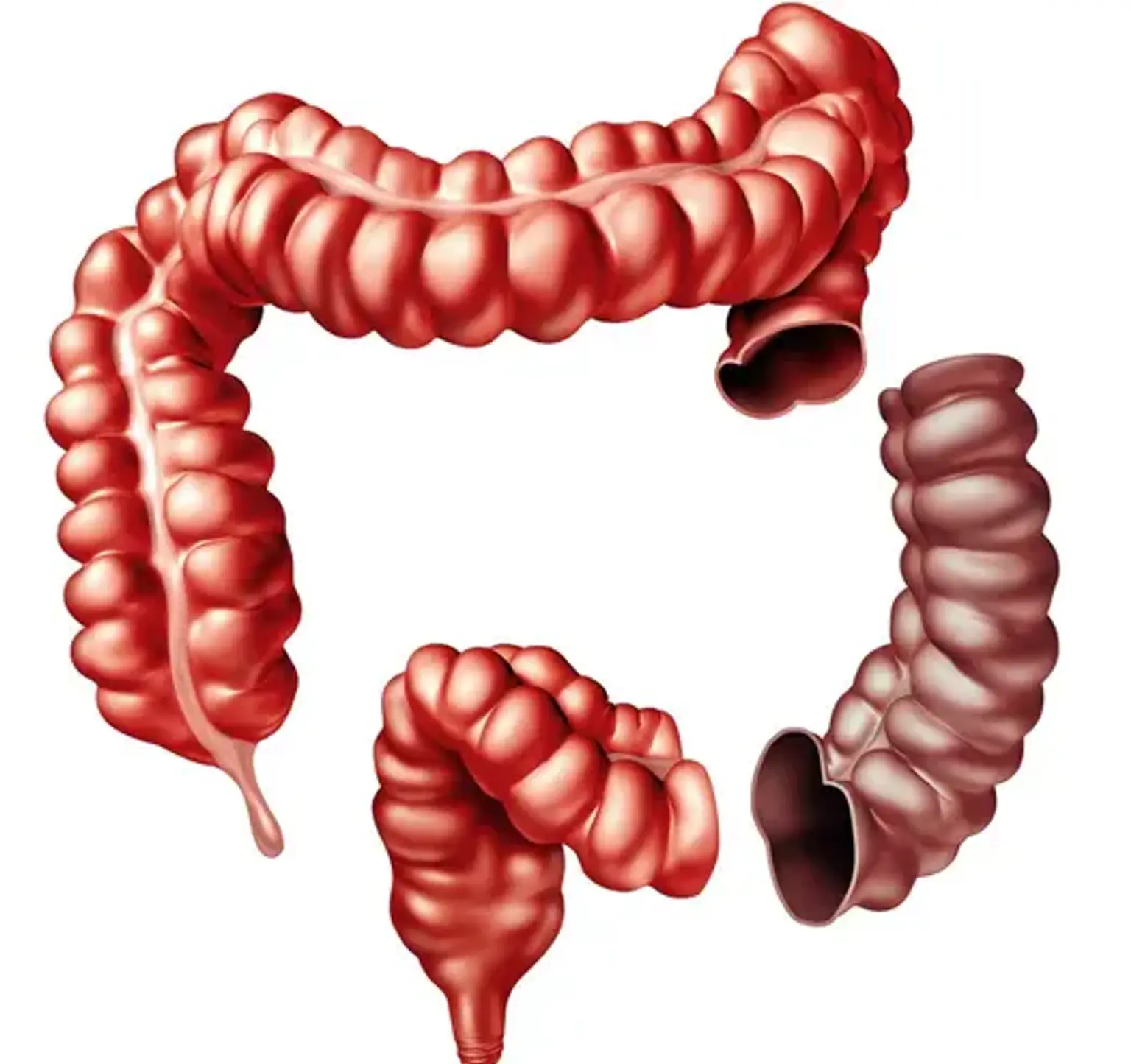
Your colon is a part of your large intestine where waste from your digesting hardens into stool. Your large intestine extends after your colon into your rectum and anus, where food waste departs your body.
A colectomy is a surgical procedure that removes all or part of your colon. It is also known as colon resection surgery. Because your colon is a portion of your large bowel, colectomy is a form of big bowel resection.
For a variety of reasons, you may need to have part or all of your colon removed. Cancers and diseases that cannot be treated with drugs are examples of this. Removing the damaged section allows the rest of your gastrointestinal tract to operate normally.