Stroke
Overview
Cerebrovascular accidents, often known as strokes, are common across patient populations and can be a major cause of morbidity and mortality. Strokes are classified as either ischemic, hemorrhagic, or subarachnoid. Understanding your stroke can help you understand how your brain operates.
What is a stroke?
A stroke, also known as a cerebrovascular accident or CVA, occurs when part of the brain loses blood flow and the area of the body controlled by the blood-deprived brain cells stops operating. This blood supply loss can be ischemic (lack of blood flow) or hemorrhagic (bleeding into brain tissue)
A stroke is considered a medical emergency since it might result in death or severe disability. There are therapeutic options for ischemic strokes, but they must be initiated within the first few hours of the onset of symptoms. If a stroke is suspected, the patient, family, or onlookers should dial 9-1-1 and activate emergency medical assistance immediately.
A transient ischemic attack (TIA or mini-stroke) is a brief ischemic stroke in which the symptoms disappear on their own. This circumstance also necessitates an immediate examination in order to reduce the danger of a future stroke. A stroke is classed as a TIA if all symptoms have disappeared within 24 hours.
What are the types of stroke?
Strokes are often categorized according to the mechanism that caused the loss of blood flow, either ischemic or hemorrhagic. A stroke can also be classified according to which portion of the brain was injured (for example, a right temporal stroke) and which part of the body ceased operating (stroke affecting the left arm).
Ischemic stroke
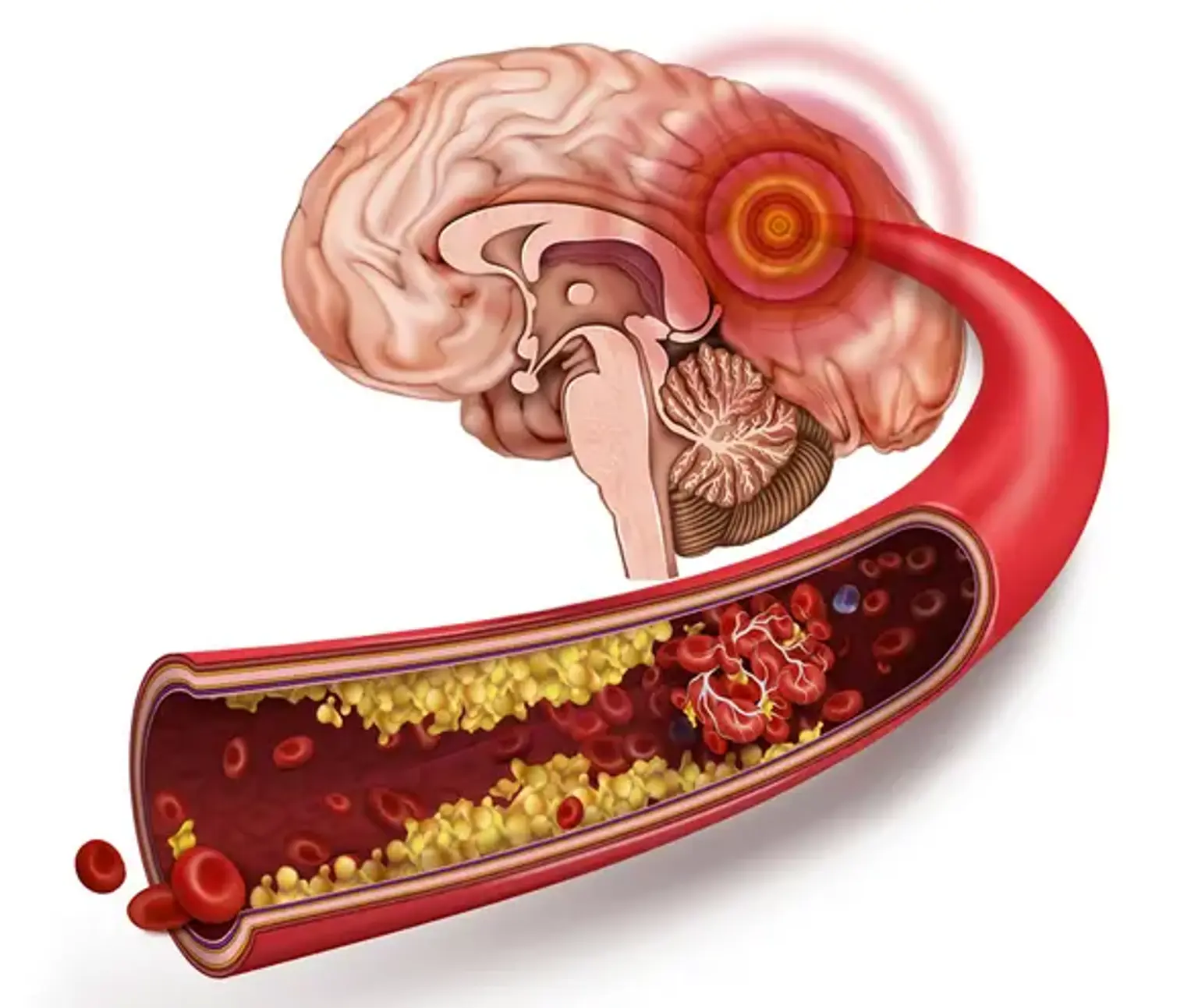
An ischemic stroke occurs when an artery in the brain becomes obstructed or blocked, preventing oxygen-rich blood from reaching brain cells. The artery can get obstructed in a variety of ways. An artery can constrict over time due to cholesterol deposition, known as plaque, in a thrombotic stroke. If the plaque ruptures, a clot forms at the location, preventing blood from getting to brain cells downstream, depriving them of oxygen.
An embolic stroke occurs when an artery becomes blocked due to debris or a clot that moves from the heart or another blood vessel. An embolus, also known as an embolism, is a clot, a piece of fatty material, or another substance that travels through the circulation and becomes lodged in a blood artery, causing a blockage.
Blood clots that embolize often form in the heart. The most prevalent cause of these blood clots is atrial fibrillation, a cardiac arrhythmia in which the top chambers of the heart, the atria, do not beat in an orderly rhythm. Instead, the atria wobble like a bowl of Jell-O due to the erratic electrical pattern. While blood continues to flow to the ventricles (the lower chambers of the heart) to be pumped to the body, some blood can form minute blood clots along the inner walls of the atrium. If a clot breaks off, it can travel to the brain and obstruct blood flow to a specific area of the brain, resulting in a stroke.
The carotid arteries are two big blood channels that deliver blood to the brain. With the accumulation of cholesterol plaque, these arteries might constrict or develop stenosis. The plaque's surface is uneven, and debris can break off and embolize into the brain, blocking blood veins downstream and depriving brain cells of oxygen-rich blood.
Hemorrhagic stroke
When a blood artery ruptures and spills blood into brain tissue, the brain cells cease to function. The bleeding or hemorrhage is frequently caused by poorly regulated high blood pressure, which damages the arterial wall over time. An aneurysm, a congenital weakening or bulging of an artery wall, or an AVM (arteriovenous malformation), a congenital anomaly in which an artery and vein link inappropriately, can also cause blood to flow. The bleeding can generate a hematoma, which directly destroys brain cells, as well as swelling, which puts more strain on surrounding brain tissue.
Describing a stroke by anatomy and symptoms
Four major arteries supply the brain with blood:
- The right and left carotid arteries
- The right and left vertebral arteries
- The carotid and vertebrobasilar arteries combine to create the Circle of Willis near the base of the brain, and arteries branch off from this circle to deliver blood to the brain.
The right side of the body is controlled by the left side of the brain and vice versa. Speech is usually placed in the dominant hemisphere, which is the left brain. The blood supply to the front two-thirds of the brain, including the frontal, parietal, and temporal lobes, is provided by the anterior and middle cerebral arteries. These regions of the brain are in charge of voluntary body movement, sensation, speech and cognition, personality, and conduct.
The vertebral and basilar arteries are part of the posterior circulation and supply the occipital lobe, which regulates vision, the cerebellum, which governs coordination and balance, and the brainstem, which controls unconscious brain processes like as blood pressure, respiration, and alertness.
Strokes can be classified according to the function of the body that is lost as well as the location of the brain that is damaged. Most strokes involving the brain cause symptoms on either the right or left side of the body. Symptoms of a stroke that affects the brainstem or the spinal cord may appear on both sides of the body.
Strokes can impair motor function, or the body's capacity to move. A part of the body, such as the face, hand, or arm, may be affected. A complete side of the body may be affected (for example, the left part of the face, left arm, and left leg). Hemiparesis (Hemi = half + paresis = weak) refers to weakness on one side of the body, whereas hemiplegia (Hemi = half + plegia = paralysis) refers to paralysis.
Sensory function, or the capacity to feel, can also impact the face, hand, arm, trunk, or a combination of these.
Other symptoms such as speech, vision, balance, and coordination assist in locating the portion of the brain that has ceased working and aid in the clinical diagnosis of stroke. This is an important topic to understand since not every loss of neurologic function is caused by stroke, and if the anatomy and physiology do not match the loss of physical function, alternative illnesses that can impact both the brain and the body may be explored.
What causes a stroke?
Thrombotic stroke
The most common cause of a stroke is a clot blocking an artery in the brain (thrombosis). The blood and oxygen supply to the area of the brain supplied by the blocked blood artery is subsequently cut off. As a result of the lack of blood and oxygen, the cells in that area of the brain die, and the part of the body it regulates ceases to function. A cholesterol plaque in one of the brain's tiny blood arteries usually ruptures and initiates the clotting process. The risk factors for brain blood vessel narrowing are the same as those for heart blood channel narrowing and heart attack (myocardial infarction). These risk factors are as follows:
- High blood pressure (hypertension),
- High cholesterol,
- Diabetes, and
- Smoking.
Embolic stroke
Another form of stroke can develop when a blood clot or a piece of atherosclerotic plaque (cholesterol and calcium deposits on the interior of the heart or artery) breaks off, travels through the circulation, and becomes lodged in a cerebral artery.
When blood flow is interrupted, brain cells are deprived of the oxygen and glucose they need to operate, and a stroke develops. An embolic stroke is the medical term for this type of stroke. A blood clot, for example, may develop in the heart chamber as a result of an abnormal heart rhythm, such as atrial fibrillation. These clots usually remain connected to the inner lining of the heart, but they can occasionally break free, move through the circulation (embolize), block a brain artery, and cause a stroke.
An embolism, either plaque or clot, can also begin in a big artery (such as the carotid artery, a major artery in the neck that provides blood to the brain) and then proceed downwards to obstruct a tiny artery within the brain.
Cerebral hemorrhage
When a blood artery in the brain ruptures and bleeds into the surrounding brain tissue, this is referred to as a cerebral hemorrhage. A cerebral hemorrhage (brain bleeding) produces stroke symptoms by depriving areas of the brain of blood and oxygen in a number of ways. Some cells lose blood flow. Furthermore, blood is highly irritating and can induce swelling of brain tissue (cerebral edema).
Subarachnoid hemorrhage
A subarachnoid hemorrhage occurs when blood collects behind the arachnoid membrane that lines the brain. The blood comes from a faulty blood vessel that leaks or ruptures. This is frequently caused by an aneurysm (an abnormal ballooning out of the blood vessel)
Subarachnoid hemorrhages are typically associated with a severe headache, nausea, vomiting, light sensitivity, and stiff neck. Major neurological implications, such as coma and brain death, may ensue if the condition is not diagnosed and treated.
Migraine headache
People who suffer from migraine headaches tend to have a slightly higher risk of stroke. The mechanism of migraine or vascular headaches includes constriction of the blood arteries in the brain. Some migraine headache bouts might even mirror stroke symptoms, such as loss of function on one side of the body or visual or speech issues. Usually, the symptoms go away as the headache does.
What is a transient ischemic attack (TIA)?
A transient ischemic attack (TIA, often known as a mini-stroke) is a brief stroke that improves and disappears on its own. It is a brief (less than 24 hours) period of transient impairment of brain function caused by a decrease of blood flow. A TIA results in a loss of function in the part of the body controlled by the damaged section of the brain.
A clot that develops spontaneously in a blood artery within the brain is the most common cause of a loss of blood flow to the brain (thrombosis). However, it can also be caused by a clot that originates elsewhere in the body, dislodges, and travels to lodge in a cerebral artery (emboli). Other causes of a TIA include arterial spasms and, in rare cases, a bleed into brain tissue. A TIA is sometimes referred to as a "mini-stroke" by many individuals.
A transient ischemia attack should be treated as an emergency since there is no certainty that the problem will resolve itself and function will recover on its own without medical intervention.
What are the signs and symptoms of a stroke?
The symptoms of a stroke vary depending on which part of the brain has ceased working owing to a lack of blood flow. Frequently, the patient will exhibit a number of symptoms, including the following:
- Acute change in the level of consciousness or confusion
- Acute onset of weakness or paralysis of half or part of the body
- Numbness of one half or part of the body
- Partial vision loss
- Double vision
- Difficulty speaking or understanding speech
- Difficulty with balance and vertigo
Although the symptoms of ischemic and hemorrhagic stroke are similar, people with hemorrhagic stroke may experience greater headache and vomiting.
What tests diagnose stroke?
The longer a stroke goes undiagnosed and untreated, the longer brain cells are deprived of oxygen-rich blood and the higher the number of brain cells that die and cannot be replaced.
- The American Heart Association and the American Stroke Association advise everyone to be aware of FAST when it comes to identifying stroke: Face drooping, arm weakness, difficulty speaking
- Nurses and doctors in the emergency room may utilize the National Institute of Health Stroke Scale to undertake a more thorough and standardized neurologic assessment.
A clinical diagnosis of stroke is generally made following history and physical examination by a healthcare practitioner. While timeliness is critical in reaching a diagnosis, it is equally critical to understand about the events that led to the patient's visit. For example, one patient began slurring his speech approximately an hour ago, whilst another patient has been slurring his words since last evening.
The diagnosis must be made as soon as possible, and therapy with thrombolytic medicines (clot-busting therapies) to "reverse" the stroke must be considered. The window for intervention is limited, and it may be as little as 3 to 4 12 hours following the beginning of symptoms. As a result, family members or bystanders may be required to validate facts, particularly if the patient is not completely aware or has a speech handicap.
Inquire about what symptoms are present, when they began, and if they are improving, progressing, or remaining the same. The prior medical history will search for risk factors for stroke, drugs, allergies, and any recent illnesses or procedures. Medication history is critical, especially if the patient is on anticoagulants.
A physical examination includes determining vital signs and the patient's level of alertness. A neurologic examination is undertaken, which generally includes the use of the standardized stroke scale. The heart, lungs, and abdomen are also examined.
If an acute stroke is still a possibility, blood tests and a CT scan of the head are recommended. The tests, however, are not used to determine a diagnosis but rather to aid plan treatment. Nonetheless, a CT scan is frequently utilized to distinguish between an ischemic and a hemorrhagic stroke since the treatment approaches are substantially different.
The CT scan is used to search for bleeding or tumors in the brain, as well as to determine how much brain tissue has a reduced blood supply. A CT perfusion scan, which uses an injected dye to evaluate cerebral blood flow, may also be performed to determine how much brain is at danger (perfusion). An MRI of the brain may be indicated, although this technique is not widely available in many institutions.
A complete blood count (CBC) to measure red blood cell count and platelets, electrolytes, blood glucose, and kidney function, as well as blood tests to measure blood clotting function, international normalized ratio (INR), prothrombin time (PT), and partial thromboplastin time (PTT), are all examples of blood tests. Other blood tests may be recommended depending on the patient's individual condition.
An EKG may be conducted to assess the pace and rhythm of the heart. A heart monitor is frequently put on the patient.
What is the treatment for stroke?
A stroke is a medical emergency, but fast treatment can restore blood circulation to the brain if stroke sufferers seek treatment as soon as possible.
The initial focus, as in many situations, is the CABs (Circulation, Airway, and Breathing, according to the current CPR standards) to ensure that the patient has blood flowing, no airway blockage, and can breathe, followed by proper blood pressure management. The brain's capacity to control respiration, blood pressure, and heart rate may be lost in severe strokes, particularly those involving the brainstem.
Intravenous lines will be placed in patients, oxygen will be provided, blood tests will be conducted, and noncontrast CT scans will be performed. Simultaneously, the health care professional evaluates the clinical diagnosis of stroke and decides whether thrombolytic therapy (tPA, a clot-busting medication) or clot retrieval (mechanically removing the clot through catheters threaded into the blocked artery) is an option for treating the stroke.
- How stroke is treated?
If an ischemic stroke has been diagnosed, there is a window of time during which thrombolytic treatment with tPA (tissue plasminogen activator) may be an option. tPA removes the clot that is obstructing a cerebral artery and restores blood flow.
Hemorrhagic strokes are tough to treat, thus it's critical to see a specialist (neurosurgeon) almost once to see whether the patient has any therapeutic alternatives (possibly aneurysm clipping, hematoma evacuation, or other techniques). In contrast to ischemic strokes, hemorrhagic strokes are not treated with tPA or other thrombolytic medicines since they might exacerbate bleeding, aggravate hemorrhagic stroke symptoms, and cause mortality. As a result, before beginning therapy, it is critical to distinguish between a hemorrhagic stroke and an ischemic stroke.
- How many stroke patients receive tPA?
The choice to give tPA to the right patient (there are various reasons why the medicine is not advised even if the patient comes on time) is one that health care providers debate with the patient and family because tPA has the potential of causing brain hemorrhage. While there is a potential advantage, because blood vessels are frail, there is a 6% chance that an ischemic stroke will progress to a hemorrhagic stroke with a brain hemorrhage. This danger is reduced if the medicine is administered early and a suitable patient is chosen.
Some stroke patients are eligible for mechanical thrombectomy, which involves inserting a tiny catheter into the blocked artery in the neck or brain and sucking the clot out. Mechanical thrombectomy may be considered up to 24 hours after the beginning of symptoms, depending on the patient, the extent of the stroke, the location of the blockage in the brain, and brain function. Mechanical thrombectomy is not accessible in many hospitals and is not suitable for all patients. These operations need the expertise of an interventional neuroradiologist, neurologist, or neurosurgeon.
When tPA and other therapies are not feasible or required, the patient is frequently admitted to the hospital for monitoring, supportive care, and referral for rehabilitation.
Endovascular treatment
Mechanical thrombectomy, or the removal of the blood clot that is causing the ischemic stroke, is a viable therapy for the blockage of a big artery, such as the middle cerebral artery. This technique is safe and effective if performed within 12 hours of the beginning of symptoms. It did not decrease the risk of mortality, but it did lower disability when compared to intravenous thrombolysis, which is commonly used in persons being assessed for mechanical thrombectomy. Thrombectomy may be beneficial in certain situations up to 24 hours following the beginning of symptoms.
Craniectomy
Strokes that damage substantial areas of the brain can result in considerable brain edema as well as subsequent brain injury in the surrounding tissue. This syndrome is most common in strokes that injure brain tissue that is dependent on the middle cerebral artery for blood flow, and it is also known as "malignant cerebral infarction" due to the poor prognosis. Medication may be used to relieve the pressure, but some patients require hemicraniectomy, which is the temporary surgical removal of the skull on one side of the head. This reduces the likelihood of mortality, yet some people who would have died otherwise live with disabilities.
What is the prognosis for a person that suffers a stroke?
Stroke is still a leading cause of death in the United States and across the world. In the United States, 20% of stroke victims die within a year. The objective, given the capacity to intervene with thrombolytic treatment to reverse the stroke and more vigorous rehabilitation, is to enhance patient survival and function following recovery.
Hospitals with specialists, equipment, and resources to respond immediately and aggressively in stroke treatment have been found to improve stroke survival as well as patient function and recovery. Knowing which hospitals in your region are designated stroke centers will benefit you since they will have the expertise and equipment needed to reduce diagnosis-to-treatment timelines.
Many difficulties might arise in stroke patients, and some may be unable to return to full-time job due to disability. Patients have physical symptoms such as diminished body function, mental symptoms such as impaired cognition, and emotional symptoms such as depression and anxiety.
Return to function is determined by the degree of the stroke, the portions of the brain and body that have stopped working, and any problems that emerge. Patients who have lost their capacity to swallow may get aspiration pneumonia, which occurs when they inhale food or saliva into their lungs and become infected. Patients who have trouble moving may develop pressure sores and infections as a result of skin disintegration.
Up to 10% of individuals may experience seizures as a consequence. Seizures are more likely to occur if the stroke is severe.
Is recovery after a stroke possible?
Prompt intervention in acute stroke and restoring blood flow to brain tissue improve the chances of stroke patients being saved and brain damage being reduced. In patients who suffer physical, mental, and emotional disabilities as a result of a stroke, rehabilitation provides the promise of improved function and a return to pre-stroke levels of activity.
Again, prevention and lowering risk factors for not only stroke but also heart attack and peripheral vascular disease (PAD) are the best stroke treatments.
Conclusion
A stroke occurs when blood flow to a portion of the brain is suddenly interrupted, causing it to cease working and eventually damage brain cells. During a stroke, the cells in the afflicted portion of the brain begin to die, and that part of the brain becomes unable to function correctly. This can impair a person's ability to walk, talk, eat, see, read, socialize, or perform tasks that they were able to perform before to the stroke. Many stroke victims have weariness as well as difficulties remembering, understanding, or thinking clearly.