Introduction
Tonsil removal surgery, also known as tonsillectomy, is a common procedure that removes the tonsils, typically due to chronic infections, enlarged tonsils, or breathing problems like sleep apnea. This surgery helps alleviate discomfort caused by recurrent tonsillitis, sore throats, and other complications related to tonsil health.
Tonsillectomy can be performed in both children and adults, though it is more common in children who suffer from frequent throat infections. Korean tonsil surgery has gained popularity for its advanced techniques, minimal complications, and high recovery success rates, making it a favored choice for many international patients seeking effective treatment.
What Are Tonsils and Why Are They Removed?
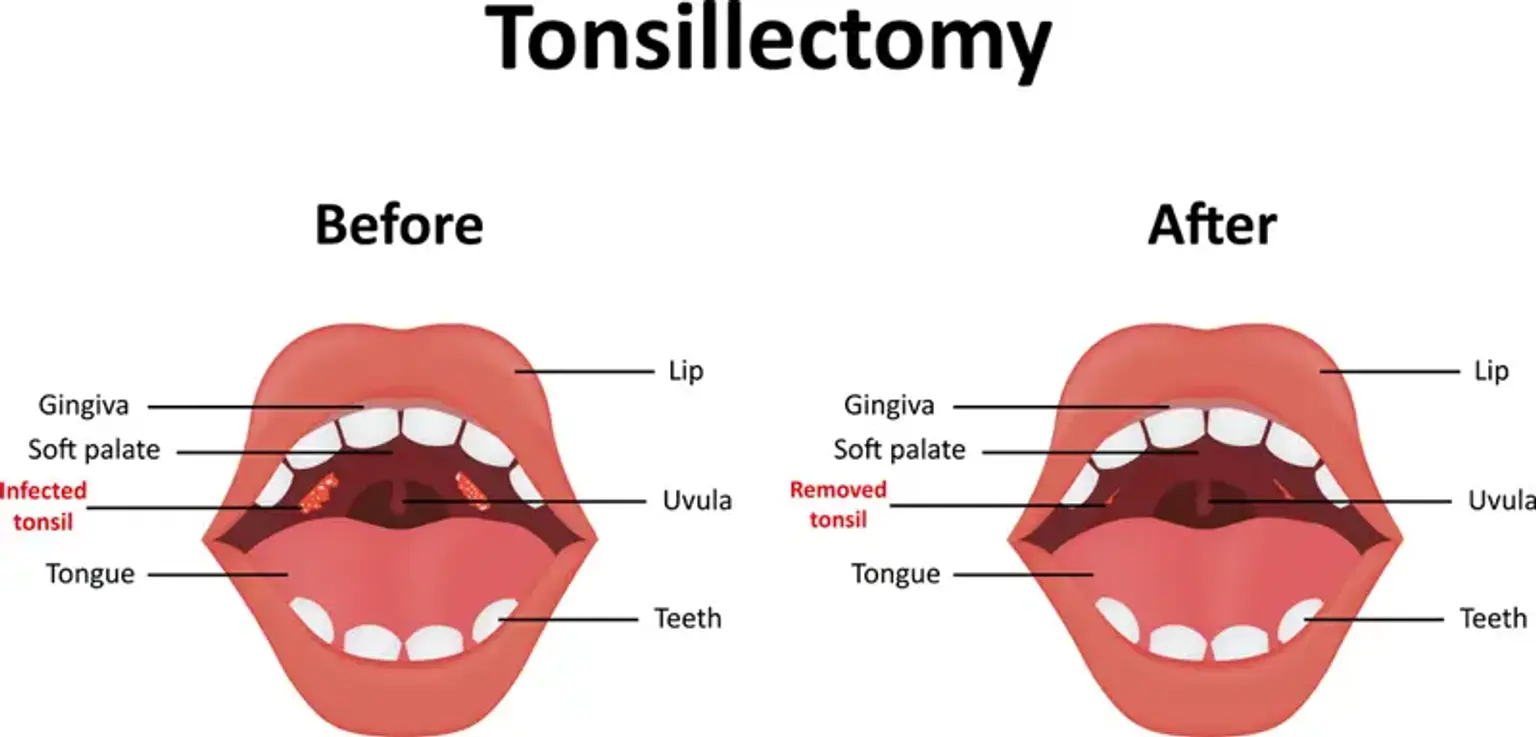
The tonsils are two small glands located at the back of the throat that play a role in the immune system by fighting infections. However, in some cases, tonsils can become a source of frequent infections, leading to the need for removal.
Tonsils may become enlarged due to infection or chronic inflammation, and this can lead to issues such as difficulty swallowing, frequent sore throats, and even problems with breathing, particularly in children with sleep apnea. Tonsil removal surgery addresses these health concerns and can provide long-term relief by removing the source of recurring infections and alleviating symptoms.
How Is Tonsil Removal Surgery Performed?
Tonsil removal surgery involves the removal of the tonsils through the mouth, and it is typically performed under general anesthesia. There are two main methods for performing tonsillectomy:
Traditional surgery: The surgeon removes the tonsils through the mouth using surgical tools, which may require a longer recovery time.
Laser tonsillectomy: A minimally invasive procedure using a laser to remove the tonsils, offering benefits like reduced bleeding, faster recovery, and less pain.
After the surgery, the incision sites are typically cauterized to prevent bleeding, and the patient will be monitored as they wake from anesthesia. The recovery process can vary depending on the method used and the patient's age and overall health.
For those considering tonsillectomy in Korea, the surgery is performed using modern techniques that ensure a higher success rate, minimal discomfort, and a quick recovery.
Tonsillectomy Risks and Complications
While tonsillectomy is generally a safe procedure, there are some risks and potential complications to consider. These can include:
Infection: Infection at the surgical site can occur, though it is rare. Proper care, including maintaining a clean mouth and avoiding germs, is essential to prevent this.
Bleeding: A small amount of bleeding can occur after surgery, but excessive bleeding may require immediate medical attention.
Pain: While some pain is expected, it should be manageable with medication. If the pain is severe or persistent, it may indicate a complication.
Dehydration: Difficulty swallowing can lead to dehydration, especially in children, so staying hydrated is key during recovery.
The risk of complications is minimized with proper surgical techniques, and experienced surgeons, such as those performing tonsillectomy in Korea, take every precaution to ensure the patient’s safety. Surgeons in Korea also use modern technologies that minimize risks and improve outcomes, ensuring the procedure’s success.
Tonsil Removal for Aesthetic Concerns
In addition to improving health, tonsil removal surgery can also have aesthetic benefits. Enlarged tonsils or tonsils that are frequently infected may lead to a swollen appearance in the neck area. For some patients, the visible lump can be a source of self-consciousness, especially in younger individuals or those in public-facing roles. Tonsil removal for aesthetic concerns can help reduce the prominence of the neck area, creating a more streamlined and youthful appearance.
While tonsil surgery is primarily done for medical reasons, patients often find that the procedure also boosts their confidence. The ability to eliminate the visible bulge associated with enlarged tonsils can be an added benefit, particularly for those considering surgery for cosmetic purposes. In countries like Korea, where aesthetic considerations are often integrated into medical treatments, tonsillectomy procedures are tailored to address both health and cosmetic needs.
Sleep Apnea and Tonsils: How Tonsil Removal Helps
Enlarged tonsils can be a major contributor to sleep apnea, a condition where the airway is obstructed during sleep, leading to interrupted breathing and poor-quality rest. Tonsil removal surgery for sleep apnea is particularly effective in children, where enlarged tonsils often cause significant airway obstruction. By removing the tonsils, the patient can experience improved airflow and a reduction in sleep disturbances.
For adults, tonsil removal surgery can also be beneficial for those with obstructive sleep apnea caused by enlarged tonsils or adenoids. The removal can alleviate symptoms like snoring, daytime fatigue, and difficulty concentrating.
After tonsillectomy, many patients report a significant improvement in their sleep quality. The reduction in airway blockage leads to deeper, more restful sleep. Korean hospitals, known for their expertise in both medical and cosmetic procedures, frequently perform tonsillectomies for sleep apnea with great success, ensuring improved breathing and sleep patterns post-surgery.
Tonsil Removal Surgery: Indications for the Procedure
Tonsillectomy is often recommended when a person experiences repeated infections (often referred to as chronic tonsillitis), obstructive sleep apnea, or severe tonsil enlargement that causes discomfort and difficulty breathing. Here are common reasons for undergoing tonsil removal surgery:
Chronic tonsillitis: Frequent, painful throat infections that don’t respond to antibiotics.
Sleep apnea: Enlarged tonsils may block the airway, leading to disrupted sleep.
Enlarged tonsils: When tonsils become large enough to affect swallowing or breathing.
Aesthetic concerns: Some individuals seek surgery for cosmetic reasons, as enlarged tonsils can affect the appearance of the throat.
This surgery is also beneficial for people who suffer from tonsil infections that disrupt daily life or interfere with general well-being.
Tonsillectomy in Children vs. Adults
Tonsil removal surgery is performed on both children and adults, but the approach and recovery can vary slightly depending on the age of the patient.
Tonsil removal in children: Children often recover faster than adults and are generally able to return to normal activities after about a week. However, they may require extra support during the first few days, especially for pain management and hydration. Parents should ensure their child follows post-operative care instructions carefully to prevent complications.
Tonsil removal in adults: Adults may experience a slightly longer recovery period due to differences in healing rates. The pain following surgery can be more pronounced in adults, and they might need a longer time to fully recover. Despite these differences, the procedure is just as effective for adults and can lead to a significant improvement in health and well-being.
In Korea, experienced surgeons understand the unique needs of both children and adults, ensuring a smooth and efficient procedure for patients of all ages. The post-operative care in Korean hospitals is tailored to each age group, improving comfort and reducing recovery time.
Post-Tonsillectomy Care
Proper post-tonsillectomy care is crucial for a smooth recovery. After surgery, it’s important to avoid any actions that could irritate the throat, such as vigorous coughing, swallowing hard foods, or engaging in physical activity. Here are a few essential tips:
Pain management: Pain and discomfort can be expected for a few days after surgery. Pain relievers prescribed by the doctor should be taken as directed to manage symptoms effectively.
Hydration: Drink plenty of fluids like water or clear juices. Staying hydrated helps with healing and reduces the risk of bleeding.
Diet: Stick to a soft or liquid diet during the first few days. Avoid spicy, hard, or crunchy foods that could irritate the healing tissue.
Rest: Rest is essential for healing, so ensure that the patient gets adequate sleep and avoids any strenuous activity.
In Korean tonsil surgery, healthcare providers give clear, detailed post-operative instructions, making recovery easier to manage and ensuring that complications are avoided.
Tonsil Removal Surgery Benefits
The benefits of tonsil removal surgery extend beyond just eliminating a physical problem. Here are some of the main advantages:
Prevention of recurrent infections: Tonsil removal significantly reduces the frequency and severity of throat infections, such as tonsillitis.
Improved sleep: For individuals with sleep apnea caused by enlarged tonsils, surgery can lead to better, more restful sleep.
Easier breathing: Enlarged tonsils can obstruct the airway, leading to difficulty breathing, especially during sleep. Removing them can restore normal breathing.
Enhanced quality of life: With fewer infections and improved health, patients often experience an overall increase in energy, productivity, and well-being.
For children, tonsil removal can prevent missed school days, while adults experience fewer sick days and less discomfort. Many patients also notice a significant improvement in facial volume restoration when their enlarged tonsils are removed, especially if they were causing visible swelling. In Korea, tonsillectomy is known for its high success rate, and patients often report significant improvements in their quality of life after the procedure.
Cost of Tonsil Removal Surgery in Korea
The cost of tonsil removal surgery varies depending on factors such as the type of procedure, the complexity of the case, and the hospital or clinic performing the surgery. On average, tonsillectomy in Korea tends to be more affordable compared to Western countries, especially considering the high quality of healthcare available. The cost typically includes the surgery itself, anesthesia, post-operative care, and follow-up appointments.
For international patients, tonsil surgery in Korea is often a cost-effective solution, providing high-quality care with state-of-the-art medical facilities at a fraction of the price found in other countries. Many hospitals offer packages for international patients that include travel and accommodation arrangements, making it easier for people from around the world to access world-class medical care.
For those concerned about tonsillectomy cost in Korea, it is worth noting that the affordability, combined with the expertise of Korean surgeons, makes it an appealing destination for tonsil removal surgery.
Minimally Invasive Tonsil Removal Surgery
Minimally invasive tonsil surgery has become a popular option for patients seeking tonsil removal due to its reduced recovery time and lower risk of complications. This technique uses specialized tools and methods, such as laser or coblation technology, to remove the tonsils through smaller incisions or even through the mouth with no external cuts. Laser tonsillectomy is one of the most common minimally invasive techniques, offering the advantage of reduced bleeding, less pain, and faster recovery compared to traditional methods.
The key benefit of minimally invasive tonsil removal surgery in Korea is the high level of expertise available. Korean surgeons use the latest technologies to ensure that the procedure is as gentle as possible while still being highly effective. This approach not only shortens the hospital stay but also ensures a smoother post-operative experience, making it an excellent choice for both children and adults.
Laser Tonsillectomy Procedure in Korea
Laser tonsillectomy is a cutting-edge technique that uses focused laser light to remove the tonsils. The laser cauterizes tissue as it cuts, reducing bleeding and minimizing the risk of infection. This method can result in a quicker recovery time and less discomfort compared to traditional surgical methods, making it an appealing option for many patients.
In Korea, laser tonsillectomy has gained popularity due to the country’s advanced medical technologies and highly skilled surgeons. Korean hospitals specialize in laser tonsillectomy procedures, offering patients the benefits of reduced recovery time, minimal scarring, and less postoperative pain. Many international patients are drawn to Korea for laser tonsillectomy because of the high success rate and the affordable costs associated with these advanced treatments.
Tonsillectomy Recovery: What to Expect
Recovery after tonsil removal surgery typically takes about 7 to 10 days, though it can vary depending on the individual. The first few days post-surgery are often the most uncomfortable due to pain and swelling in the throat. During this time, it’s important to follow the surgeon’s aftercare instructions carefully to ensure proper healing.
Tonsillectomy recovery includes managing pain with prescribed medications, drinking plenty of fluids to stay hydrated, and consuming soft foods to prevent irritation at the surgical site. Most patients will feel better within a week, but it’s important to rest and avoid strenuous activities during the recovery period. The complete healing process can take up to two weeks.
For children, recovery tends to be smoother, though they may need additional support for comfort during the first few days. In Korea, hospitals are equipped with advanced post-operative care techniques to ensure a faster recovery and manage any complications, offering a comprehensive support system to guide patients through the recovery process.
Tonsillectomy in Korea: Why It’s Popular
Tonsillectomy in Korea has become increasingly popular, especially among international patients, due to the country's reputation for high-quality healthcare, state-of-the-art medical facilities, and skilled surgeons. Korean hospitals have a track record of performing tonsil removal surgery with great success, offering a variety of advanced techniques like minimally invasive tonsil surgery and laser tonsillectomy to suit each patient's needs.
The affordability of tonsillectomy in Korea compared to Western countries is another driving factor for patients considering medical tourism. Many hospitals in Korea also provide comprehensive packages that include travel, accommodation, and post-surgical care, making it easier for international patients to access top-tier healthcare. Korean surgeons specialize in customizing treatment plans, ensuring that each patient receives the most effective and comfortable care.
Risks of Tonsillectomy Surgery
While tonsillectomy surgery is generally safe, it is important to be aware of the potential risks and complications that can arise. These include:
Infection: As with any surgery, there is a risk of infection, especially if the surgical site is not kept clean or if post-operative care instructions are not followed properly.
Bleeding: Some bleeding is common after surgery, but excessive bleeding may require further medical intervention.
Pain: Although pain is expected, especially in the first few days after surgery, it is typically manageable with pain relief medications. For some, however, the pain can persist longer.
Scarring: There may be scarring around the surgical area, although in laser tonsillectomy, scarring is minimized.
By following proper post-tonsillectomy care and being aware of potential risks, complications can be minimized. In Korea, experienced surgeons take every precaution to ensure the safest procedure possible, and healthcare professionals provide thorough post-operative monitoring to ensure proper recovery and minimize risks.
Tonsillectomy for Chronic Tonsillitis Treatment
Tonsillectomy is often the most effective treatment for individuals suffering from chronic tonsillitis. Chronic tonsillitis refers to the frequent inflammation and infection of the tonsils, leading to sore throats, fever, and difficulty swallowing. For patients who experience repeated infections despite using antibiotics, tonsil removal surgery can provide a long-term solution by eliminating the source of infection.
By removing the tonsils, tonsillectomy not only prevents further infections but also reduces the overall burden of throat pain and discomfort. In children, this can also improve their overall health and quality of life, as they no longer have to endure constant infections. In Korea, where medical advancements ensure effective and minimally invasive techniques, the tonsillectomy procedure has become a standard and highly successful treatment for chronic tonsillitis.
What to Expect During Tonsil Removal Surgery
Before undergoing tonsil removal surgery, patients typically go through a pre-surgical consultation, where their medical history and current health status are reviewed. This helps the surgeon determine the most suitable type of surgery and anesthesia. On the day of surgery, general anesthesia is administered, and the surgeon proceeds with either traditional or laser tonsillectomy to remove the tonsils.
The surgery itself typically takes about 30 minutes to an hour. During the procedure, the surgeon may use different tools or lasers to remove the tonsils, with the goal of minimizing bleeding and ensuring the safest approach. After surgery, patients are monitored for a few hours to ensure there are no immediate complications. While the procedure is generally safe, patients should expect some discomfort and pain during the recovery process.
In Korean tonsil surgery, hospitals utilize advanced monitoring equipment and experienced surgical teams to ensure the procedure goes smoothly, and recovery is as comfortable as possible.
Frequently Asked Questions (FAQs) About Tonsil Removal Surgery
Q: How long does it take to recover from tonsil removal surgery?
A: The typical recovery time for tonsillectomy is about 7 to 10 days. However, full recovery can take up to two weeks, especially for adults, who may experience a longer healing period.
Q: Is tonsil removal surgery painful?
A: Some pain and discomfort are expected after the procedure, especially during the first few days. Pain management medications are prescribed to help alleviate this. The pain usually subsides within a few days.
Q: Can tonsils grow back after surgery?
A: In rare cases, tonsils may partially grow back, but this is uncommon after a complete tonsillectomy. Surgeons take care to ensure that all the tonsil tissue is removed to reduce the risk of recurrence.
Q: Are there any risks associated with tonsillectomy surgery?
A: While complications are rare, potential risks include infection, bleeding, and anesthesia complications. These risks are minimized when the surgery is performed by an experienced surgeon.
Conclusion
Tonsil removal surgery, or tonsillectomy, offers a highly effective solution for individuals suffering from chronic tonsillitis, sleep apnea, or other tonsil-related issues. The procedure is generally safe, and with the advances in surgical techniques such as laser tonsillectomy and minimally invasive tonsil surgery, recovery time and discomfort are significantly reduced.
If you are experiencing persistent throat infections, difficulty breathing, or aesthetic concerns due to enlarged tonsils, tonsil removal surgery may be the right option for you. It’s essential to consult with a qualified healthcare provider to determine whether this procedure aligns with your health needs and goals.
For those considering surgery, Korea offers world-class medical facilities and experienced surgeons who specialize in tonsillectomy, making it an excellent destination for those seeking high-quality care at affordable prices.