Introduction
Total hip replacement (THR) is a highly effective surgical procedure designed to alleviate severe hip pain and restore mobility. The surgery is typically recommended when conservative treatments, such as medication or physical therapy, no longer provide relief. Most patients undergo THR due to joint degeneration, often caused by conditions like osteoarthritis. This procedure involves removing the damaged hip joint and replacing it with a prosthetic implant.
THR is one of the most common orthopedic surgeries performed worldwide, offering patients the chance to regain their independence and improve their quality of life. It’s particularly beneficial for those who experience chronic pain and difficulty walking or performing everyday tasks.
Understanding Hip Joint Degeneration
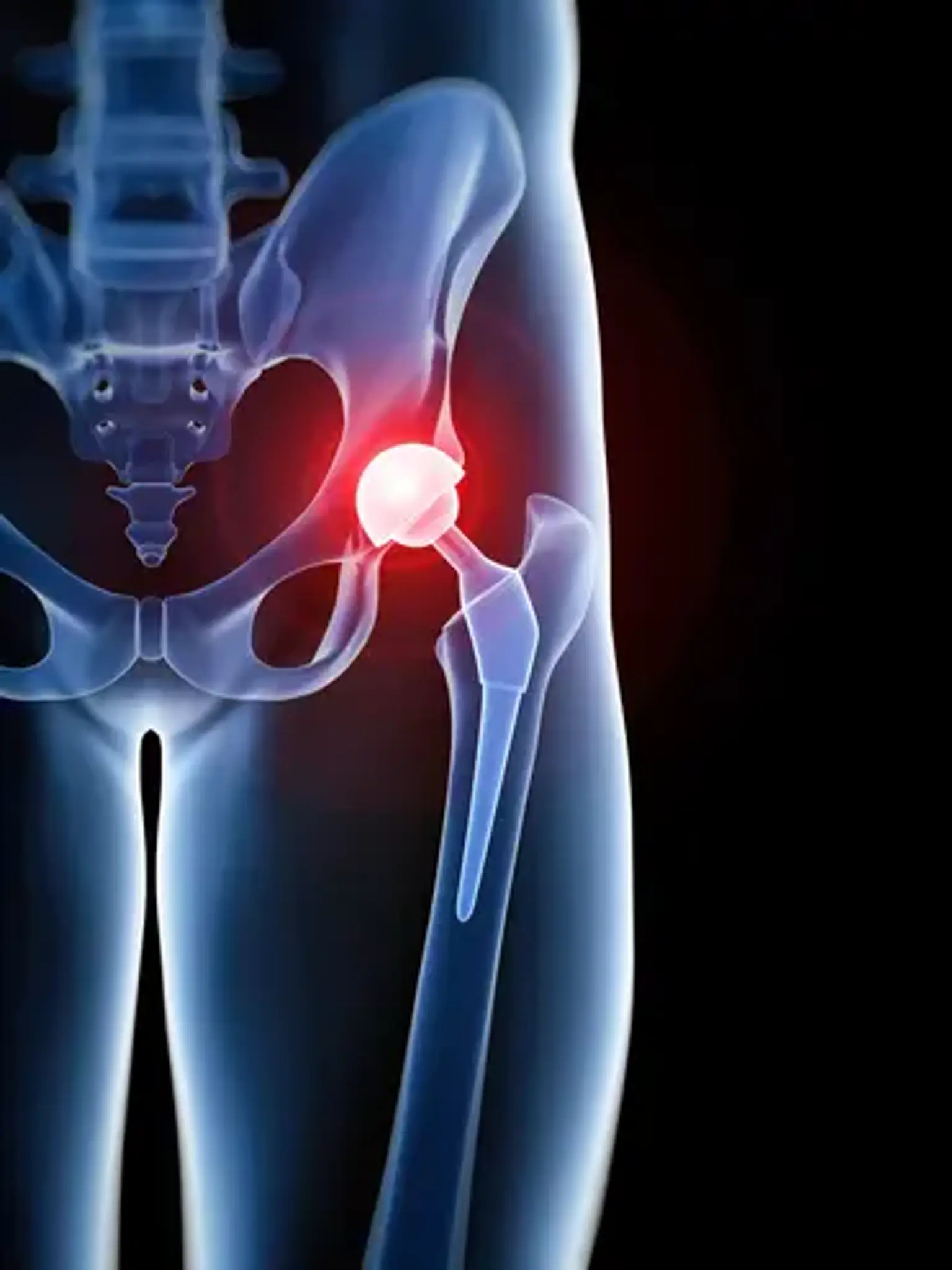
The hip joint is a ball-and-socket joint, where the femoral head (ball) fits into the acetabulum (socket) of the pelvis. When this joint becomes damaged or worn out, it can lead to significant pain and reduced movement.
Degeneration often occurs due to conditions like osteoarthritis, where the cartilage that cushions the joint breaks down. This leads to bones rubbing against each other, causing pain, stiffness, and inflammation. Other factors contributing to joint degeneration include trauma, genetic predisposition, and age. As the condition worsens, the hip joint may become so damaged that surgery is the only option for restoring mobility and relieving pain.
Conditions That May Require a Hip Replacement
The most common condition that leads to hip replacement surgery is osteoarthritis, a degenerative disease that causes the cartilage in the joint to break down. As the cartilage wears away, the bones begin to rub against each other, resulting in pain and stiffness.
Other conditions that may necessitate a hip replacement include:
Rheumatoid arthritis: An autoimmune disorder causing inflammation in the joints.
Hip fractures: Especially in older adults, when the bones break due to trauma or falls.
Avascular necrosis: A condition where blood flow to the hip bone is interrupted, leading to bone death and joint collapse.
Developmental dysplasia: A congenital condition where the hip joint doesn’t form properly, leading to wear and tear over time.
In cases where the hip joint is severely damaged and conservative treatments are ineffective, total hip replacement offers a significant improvement in quality of life.
What is Total Hip Replacement Surgery?
Total hip replacement surgery involves removing the damaged parts of the hip joint and replacing them with artificial components made of metal, plastic, or ceramic materials. The procedure aims to alleviate pain and improve joint function, making it a life-changing solution for many patients.
There are two main components of the artificial joint: a prosthetic ball (replacing the femoral head) and a socket (replacing the acetabulum). These components are designed to mimic the function of the natural hip joint, allowing for smoother movement. The procedure is typically performed under general anesthesia and can take a few hours, depending on the patient’s condition.
There are various approaches to performing THR, including traditional and minimally invasive techniques, which offer patients different options based on their individual needs.
Minimally Invasive Hip Replacement Surgery
Minimally invasive hip replacement (MIHR) is an alternative to the traditional method, offering several potential benefits:
Smaller Incisions: MIHR uses smaller incisions, typically around 3-4 inches, reducing muscle damage and leading to quicker recovery.
Reduced Pain and Blood Loss: Because the muscles around the hip are not cut as much, there is less postoperative pain and a lower risk of blood loss.
Faster Recovery: Many patients who undergo MIHR are able to leave the hospital sooner and return to normal activities more quickly.
However, not all patients are candidates for MIHR. Factors like obesity, previous surgeries, or complex joint deformities may require a traditional approach. It's important to consult with your surgeon to determine the best method for your case.
Risks and C9. Benefits of Hip Replacement Surgery
Total hip replacement offers numerous benefits for patients suffering from chronic hip pain and limited mobility. The most significant advantages include:
Pain Relief: One of the primary reasons patients opt for hip replacement is to alleviate the constant pain associated with hip joint degeneration.
Improved Mobility: After recovery, most patients regain the ability to walk, bend, and perform everyday activities with greater ease.
Better Quality of Life: The surgery often leads to a dramatic improvement in overall health, as patients can return to physical activities, exercise, and social engagements they may have previously avoided due to pain.
While the surgery has a relatively high success rate, it’s important to have realistic expectations and understand the rehabilitation process.
What to Expect During Hip Replacement Surgery
The surgery itself typically lasts about 1-2 hours. Here’s a basic overview of the process:
Anesthesia: General anesthesia (putting you to sleep) or regional anesthesia (numbing the lower body) will be used.
Incision and access: The surgeon makes an incision to access the hip joint. The damaged ball of the hip is removed, and the artificial implant is fitted.
Closing the incision: Once the prosthesis is in place, the surgeon closes the incision, and the area is stitched or stapled.
Patients are closely monitored during and after surgery to ensure stability and manage pain.
The Role of Physical Therapy in Recovery
Physical therapy plays a crucial role in the recovery process following hip replacement surgery. Starting as soon as the day after surgery, physical therapy helps patients regain strength, flexibility, and balance. Key aspects include:
Early Mobilization: The therapist will encourage light movement, such as standing and walking with assistance, to prevent complications like blood clots.
Strengthening Exercises: Targeted exercises help rebuild muscle strength around the hip joint, which is essential for long-term stability and function.
Stretching: To maintain flexibility and prevent stiffness in the new joint, stretching exercises are introduced progressively.
A personalized physical therapy plan ensures the best outcomes and helps patients return to their normal activities more quickly.
The Different Types of Hip Replacement
There are different approaches to total hip replacement (THR), with the most common being traditional and minimally invasive methods.
Traditional THR: This approach involves a larger incision (usually 8-10 inches) to provide full access to the hip joint. While effective, it typically requires a longer recovery time.
Minimally Invasive THR: This technique uses smaller incisions (about 3-4 inches) and allows for less muscle disruption. As a result, recovery may be faster, but not all patients are candidates for this method.
The choice of technique depends on various factors, including the patient's anatomy, overall health, and surgeon’s expertise. Both approaches aim for the same goal: pain relief and restored mobility.
The Cost of Hip Replacement Surgery
The cost of total hip replacement surgery can vary significantly depending on location, surgeon, hospital, and insurance coverage. On average, the procedure in the United States costs between $30,000 and $50,000, which includes hospital fees, surgeon’s fees, and rehabilitation costs. However, costs can be lower in countries with less expensive healthcare systems, such as India or Mexico.
For patients with insurance, the out-of-pocket costs may be reduced, though deductibles and co-pays will still apply. It's important for patients to discuss their insurance coverage and payment options in advance.
omplications of Hip Replacement Surgery
Like all surgeries, hip replacement carries risks, though complications are relatively rare. Possible risks include:
Infection: While sterile techniques are used, there is always a slight risk of infection.
Blood clots: Deep vein thrombosis (DVT) can occur, especially after surgery, but blood thinners and early mobilization reduce this risk.
Nerve or blood vessel injury: The hip area contains sensitive nerves and blood vessels, and injury is a potential, though uncommon, complication.
Dislocation or implant loosening: Over time, the artificial joint may wear out or shift out of place, requiring revision surgery.
Overall, the success rate for hip replacement is high, and most patients experience significant pain relief and improved mobility.
Longevity of Hip Implants
One of the most common questions patients have is, "How long will my hip replacement last?" Most modern hip implants are designed to last 15-20 years or more, though this depends on factors such as activity level, weight, and the materials used in the implant.
Material Impact: Implants made of ceramic or highly durable metals tend to last longer, while polyethylene (plastic) components may wear out more quickly.
Activity Level: Active patients who engage in high-impact sports may experience faster wear and tear, while those who lead a sedentary lifestyle may see a longer lifespan for their implant.
Revision Surgery: If an implant does wear out or become damaged, a revision surgery may be needed to replace it. This is a common and generally successful procedure, though it involves a more complex recovery.
Patients can maximize the lifespan of their implants by following the recommended post-surgery guidelines, maintaining a healthy weight, and avoiding high-impact activities.
Hip Replacement Surgery for Older Adults
Hip replacement surgery can be particularly beneficial for older adults, who are often affected by degenerative conditions like osteoarthritis. The surgery improves mobility and reduces pain, allowing elderly patients to regain independence. However, special considerations are needed for this age group:
Comorbid Conditions: Older adults often have other health issues (e.g., heart disease, diabetes) that need to be managed during the surgical process. A thorough pre-surgical evaluation is crucial.
Recovery Time: The recovery process for elderly patients may take longer, and physical therapy is essential to regain strength and mobility.
Success Rates: Studies show that hip replacement surgeries in older adults have high success rates, with most patients experiencing significant improvements in pain relief and functionality.
With proper planning and care, hip replacement surgery can dramatically enhance the quality of life for older patients.
Alternative Treatments to Hip Replacement
While hip replacement surgery is highly effective, it's important to explore alternative treatments before deciding on surgery, especially for patients who are not ready for the procedure or may not be ideal candidates. Alternatives include:
Physical Therapy: Aimed at improving strength, flexibility, and joint function, physical therapy can help manage pain and delay the need for surgery.
Injections: Corticosteroid or hyaluronic acid injections can reduce inflammation and provide temporary pain relief, though their effects are usually short-term.
Lifestyle Changes: Weight loss and low-impact exercises can reduce stress on the hip joint and slow down the degeneration process.
Hip Resurfacing: This is a less invasive alternative to total hip replacement, where only the surface of the hip joint is replaced. It is generally recommended for younger, active patients.
For some patients, these treatments may be sufficient, but for others, hip replacement may be the most effective option when conservative methods fail.
Preparing for Hip Replacement Surgery
Before undergoing total hip replacement, several preparations are necessary. Your healthcare provider will conduct a thorough evaluation, which may include:
Physical exams and imaging tests: X-rays or MRIs are used to assess the condition of your hip joint.
Blood tests and medical history: To ensure you’re healthy enough for surgery, your doctor will check for conditions like diabetes, heart disease, or infections.
Pre-surgical instructions: Patients may need to stop certain medications or adjust lifestyle habits, like quitting smoking or losing weight, to optimize surgical outcomes.
Proper preparation is key to a smooth surgery and recovery.
Choosing the Right Surgeon for Hip Replacement Surgery
Selecting the right surgeon is crucial for a successful hip replacement. Factors to consider include:
Experience and Specialization: Look for a surgeon who specializes in hip replacements and has significant experience performing the procedure. Experienced surgeons typically achieve better outcomes.
Reputation: Research the surgeon’s reputation through patient reviews, referrals from healthcare providers, or trusted organizations.
Approach and Technique: Discuss the surgical techniques they use (e.g., traditional vs. minimally invasive) and choose one that aligns with your preferences and health needs.
Communication: A good surgeon will take the time to explain the procedure, answer your questions, and help you set realistic expectations for recovery.
Choosing a qualified and trusted surgeon will significantly improve your chances of a smooth surgery and recovery.
The Global Popularity of Hip Replacement Surgery
Total hip replacement surgery has become increasingly popular worldwide, especially in countries with advanced healthcare systems like the United States, Germany, and the United Kingdom. The procedure is also gaining traction in countries like India and Mexico, where high-quality care is offered at a more affordable price.
Rising Demand: As the global population ages, the demand for hip replacement surgeries continues to increase. Many patients are seeking relief from arthritis and other degenerative conditions that limit mobility.
Medical Tourism: For those seeking lower-cost options, medical tourism for hip replacement has grown. Countries like India, Thailand, and Costa Rica offer experienced surgeons and high-quality medical care at a fraction of the cost found in Western countries.
As a result, hip replacement surgery is not only widespread but also accessible to more people globally.
Recovery Timeline After Hip Replacement
Recovery from total hip replacement varies from person to person, but a general timeline includes:
First Few Days: Patients typically stay in the hospital for 2-3 days. During this time, pain management and basic mobility exercises are the focus.
Weeks 1-6: During the first month and a half, patients gradually increase activity, with help from physical therapy. Using a walker or crutches is common during this phase.
Months 2-6: Most patients can walk independently by this stage, though physical therapy continues to improve strength and flexibility.
6+ Months: Full recovery can take anywhere from 6 months to a year. At this point, patients often return to their normal routine, though some may still experience mild discomfort during intense activities.
The recovery process is progressive, with the majority of patients experiencing significant improvement in mobility and quality of life within 3 to 6 months.
Patient Testimonials and Real-Life Success Stories
Hearing from patients who have undergone hip replacement surgery can be reassuring for those considering the procedure. Many individuals report significant improvements in their quality of life post-surgery, including:
Pain Relief: Patients who struggled with chronic hip pain often describe a dramatic reduction in discomfort, allowing them to return to daily activities and hobbies they once enjoyed.
Regained Mobility: For many, the ability to walk, climb stairs, and move freely is life-changing. People who had difficulty standing for long periods can often regain their independence.
Improved Mental Health: The relief from chronic pain and physical limitations often leads to improved mental well-being, including reduced depression and anxiety.
While each experience is unique, success stories highlight the transformative impact of hip replacement surgery on overall health and happiness.
Conclusion
Total hip replacement surgery can be life-changing for individuals suffering from debilitating hip pain and joint degeneration. While the procedure offers significant benefits, it’s essential to consider factors such as your age, overall health, and activity level before proceeding.
Consult with your orthopedic surgeon to evaluate your condition and explore the best options for your situation. With proper preparation, realistic expectations, and a commitment to post-surgery rehabilitation, most patients experience remarkable improvements in pain relief and mobility, leading to a better quality of life.
Ultimately, if conservative treatments are no longer effective, hip replacement surgery could be the key to reclaiming an active and pain-free lifestyle.