What is Eardrum Repair Surgery?
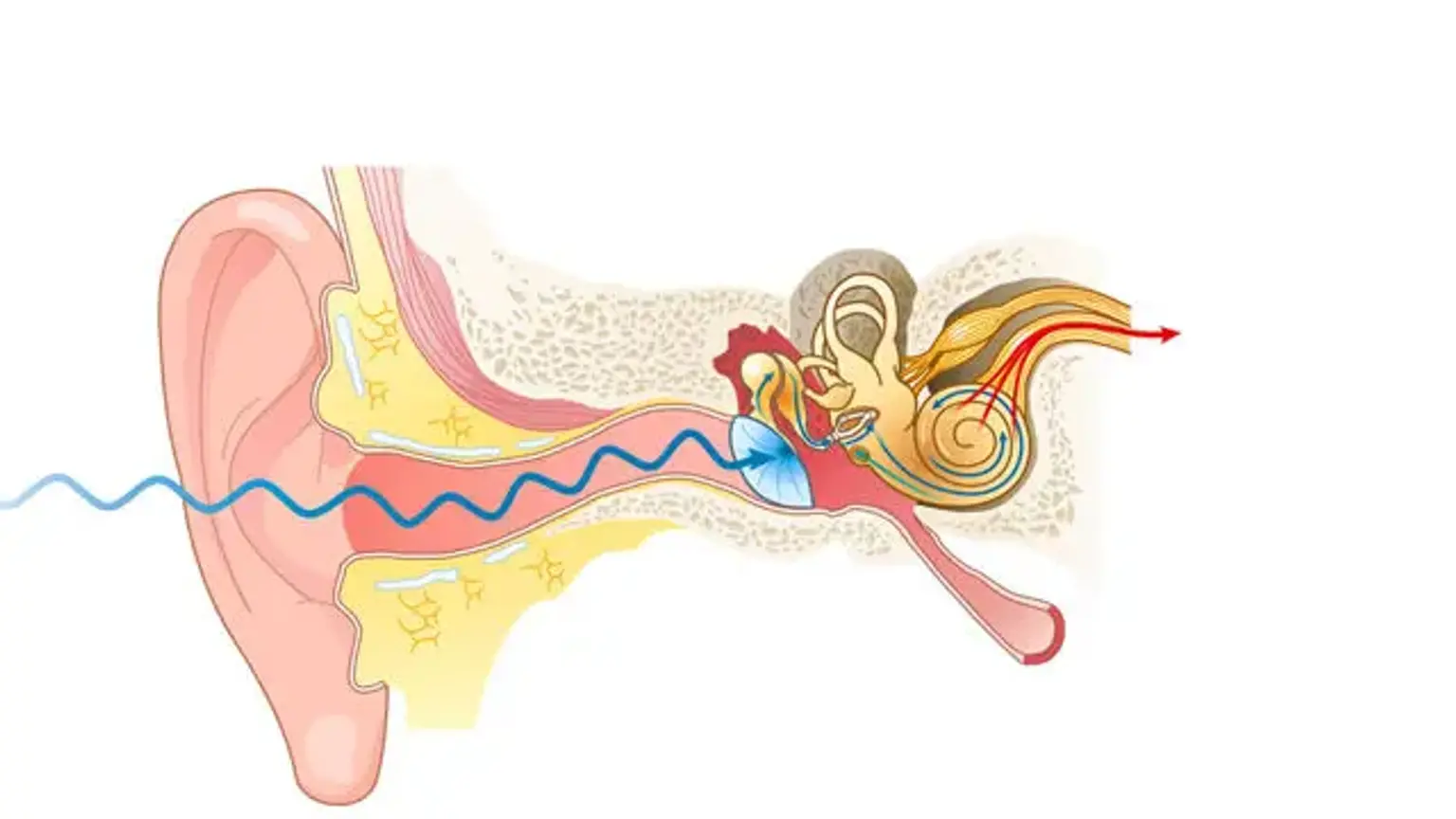
Eardrum repair surgery, also known as tympanoplasty, is a surgical procedure used to fix damage to the eardrum (or tympanic membrane), which is the thin membrane that separates the outer ear from the middle ear. This membrane plays a vital role in hearing by transmitting sound vibrations from the air to the tiny bones in the middle ear. When the eardrum is damaged due to injury, infection, or chronic ear problems, it can result in hearing loss and other complications.
Tympanoplasty aims to repair perforations (holes) or tears in the eardrum, restoring its ability to vibrate properly and transmit sound. The procedure may also address related issues, such as middle ear infections or damage to the small bones in the ear. Eardrum surgery is crucial for preventing further damage, restoring hearing, and preventing infections that could cause more severe ear-related issues in the future.
Why Eardrum Repair Surgery is Needed
Eardrum repair surgery is typically recommended for patients who have suffered from eardrum perforations or damage caused by:
Chronic ear infections: Recurrent infections can cause the eardrum to rupture or tear over time.
Trauma or injury: Physical damage from an accident or blow to the ear can perforate the eardrum.
Untreated or chronic otitis media: Infections that go untreated can result in long-term damage to the eardrum.
In cases of eardrum perforation, the damaged area no longer vibrates correctly, leading to reduced or muffled hearing. In some situations, untreated eardrum damage can lead to further complications such as chronic ear infections or hearing loss. Eardrum surgery helps to prevent these issues by sealing the perforation and restoring the eardrum’s ability to transmit sound vibrations effectively.
For many people, repairing the eardrum not only improves hearing function but also prevents recurring ear infections and helps restore normal ear pressure. This surgery is often a crucial step toward long-term ear health and the prevention of more serious ear-related issues.
Causes of Eardrum Damage
Eardrum damage can occur for several reasons, with the most common causes being infection, trauma, and chronic ear conditions.
Chronic Ear Infections: Repeated ear infections (like otitis media) can damage the eardrum over time. These infections cause fluid to build up in the middle ear, leading to pressure and eventual rupture or perforation of the eardrum.
Trauma or Injury: Direct injury to the ear, such as a blow to the head, sudden pressure changes (like during a flight), or insertion of foreign objects into the ear, can result in a tear or hole in the eardrum.
Sudden Pressure Changes: Rapid changes in air pressure, such as during air travel, scuba diving, or a blast injury, can rupture the eardrum.
Acoustic Trauma: Exposure to loud noises, such as explosions or concert-level music, can cause immediate damage to the eardrum.
Chronic Eustachian Tube Dysfunction: If the Eustachian tube (which helps equalize ear pressure) doesn’t function properly, it can lead to persistent fluid buildup, infection, and damage to the eardrum.
When the eardrum is damaged, it may not be able to transmit sound vibrations properly, leading to hearing loss. In some cases, untreated eardrum damage can also lead to chronic ear infections and discharge. Eardrum repair surgery aims to restore normal function and reduce the risk of ongoing ear problems.
Symptoms of Eardrum Damage
Damage to the eardrum can lead to several noticeable symptoms, including:
Hearing Loss: A perforated or damaged eardrum can result in partial or complete hearing loss in the affected ear. The extent of hearing loss depends on the size and location of the perforation.
Ear Pain: Patients with a ruptured eardrum may experience sharp pain in the ear, particularly during infection or trauma. This pain often subsides once the eardrum has ruptured, but it may return with infections.
Drainage from the Ear: Fluid or pus leaking from the ear, especially if there’s an active infection, is a common sign of eardrum damage.
Tinnitus: A ringing or buzzing sound in the ear, known as tinnitus, may occur due to eardrum damage.
Dizziness or Balance Problems: The eardrum and inner ear structures play a role in maintaining balance. Damage to the eardrum can lead to feelings of dizziness or unsteadiness.
In some cases, the symptoms may be mild or go unnoticed, especially if the perforation is small. However, if the symptoms persist or worsen, it’s important to seek medical attention to avoid complications and to assess whether eardrum repair surgery is necessary.
Types of Tympanoplasty Procedures
There are different types of tympanoplasty based on the size and location of the perforation, as well as the extent of damage to other structures of the ear. The most common types include:
Myringoplasty: This is a simpler procedure where the surgeon repairs a small hole in the eardrum using a graft, without involving the middle ear bones.
Type I Tympanoplasty: In this procedure, the surgeon repairs the eardrum and may also address mild damage to the middle ear, particularly when there’s a perforation but no ossicular chain (middle ear bones) damage.
Type II-III Tympanoplasty: These types are used when there’s more significant damage to the eardrum and middle ear bones. The surgeon may need to repair or replace the ossicles, allowing the sound vibrations to reach the inner ear properly.
Each type of tympanoplasty is chosen based on the severity of the damage and the individual needs of the patient. The goal is always to restore hearing function and prevent further ear infections.
Eardrum Repair Recovery
The recovery process after eardrum repair surgery can vary depending on the individual and the complexity of the procedure. Most patients can expect to spend one to two hours in the recovery room after the surgery and may go home the same day if general anesthesia was not used.
During the first few days after surgery, patients may experience some discomfort, mild pain, and a feeling of fullness in the ear. Pain can typically be managed with over-the-counter pain relievers or prescription medications. It is essential to keep the ear dry and avoid getting water in the ear canal during the initial healing period to prevent infections.
Patients should also avoid blowing their nose, which can cause pressure in the ear, and follow any instructions provided by the surgeon regarding ear care. A follow-up appointment is usually scheduled to check on healing and remove any packing that might have been placed in the ear.
Complete healing of the eardrum typically takes several weeks. It’s important to avoid strenuous activities, loud noises, and air travel during this period to ensure proper healing and to avoid complications.
Eardrum Repair Success Rate
The success rate of eardrum repair surgery is generally high, with many patients experiencing significant improvement in their hearing after the procedure. The success of the surgery depends on various factors, including the size and location of the perforation, the patient’s overall health, and how well they follow post-surgery care instructions.
In most cases, the eardrum tear repair results in successful closure of the perforation, leading to restored hearing function and prevention of further ear infections. Studies show that the success rate for tympanoplasty can range from 85% to 95%, with most patients experiencing a marked improvement in hearing.
However, the success rate can be affected by factors such as:
Extent of damage: Larger perforations or damage to the ossicles may require more complex surgery, which could affect outcomes.
Infection history: Patients with recurrent ear infections may face more challenges in healing.
Follow-up care: Adhering to post-surgical instructions is crucial for ensuring proper healing and preventing complications.
In general, the procedure has a high success rate in improving hearing, preventing further infections, and restoring ear function. With proper care, patients can expect to see long-term benefits from their eardrum repair surgery.
Eardrum Repair Surgery: The Procedure
Eardrum repair surgery, or tympanoplasty, is performed to repair a perforated or damaged eardrum. The procedure is typically done under local or general anesthesia, depending on the patient's needs and the complexity of the surgery. The goal is to close the perforation and restore the eardrum’s ability to vibrate, thus improving hearing.
The surgeon usually accesses the eardrum through the ear canal, although sometimes a small incision behind the ear is made for better access. The damaged tissue is removed, and a graft (often made from the patient’s own tissue, such as cartilage or fascia) is placed over the perforation. This graft helps seal the hole and promote healing.
In some cases, if the middle ear bones are also damaged, the surgeon may need to repair or replace the ossicles (small bones that transmit sound in the ear). This is often done at the same time as the eardrum repair, depending on the extent of the damage.
Post-Surgery Care and Eardrum Repair Recovery Timeline
After eardrum repair surgery, proper post-surgical care is essential to ensure effective healing and prevent complications. The recovery timeline varies depending on the complexity of the surgery and the patient’s adherence to aftercare instructions. However, most patients can expect the following general recovery stages:
First Few Days: You may experience mild discomfort, a feeling of fullness in the ear, and some discharge from the ear. Pain can be managed with prescribed medications. It is important to keep the ear dry and avoid getting water in it during the first week.
One to Two Weeks: During this period, you’ll need to avoid any activities that may introduce pressure into the ear, such as sneezing forcefully or blowing your nose. If you have stitches or packing in the ear, they will typically be removed during your follow-up visit.
Four to Six Weeks: The eardrum will begin to heal completely. During this time, you should avoid exposure to loud noises, vigorous physical activity, and activities that could cause pressure changes in the ear, such as flying.
Follow-up visits with your surgeon will be necessary to monitor healing. The full recovery from eardrum surgery may take anywhere from 1 to 3 months, depending on the extent of the damage and the individual’s overall health.
Eardrum Repair Surgery Cost
The cost of eardrum repair surgery varies widely depending on the location, the complexity of the procedure, and whether the surgery involves additional treatments (such as repairing the middle ear bones). In general, the cost of tympanoplasty can range from $1,500 to $4,000 in the U.S., with higher costs associated with more complex procedures.
In countries like Korea, where healthcare is renowned for both its quality and affordability, eardrum repair surgery costs may be significantly lower. Korean clinics and hospitals offer advanced surgical procedures at a fraction of the cost compared to other countries, while also maintaining high-quality standards. This has made Korea an attractive destination for patients seeking affordable and effective ear surgeries, including tympanoplasty.
Costs may also vary based on whether the procedure is performed in a hospital or a specialized clinic, as well as the surgeon’s experience and reputation. It’s important for patients to consult with healthcare providers to get a personalized estimate, including potential costs for follow-up care, medications, and any additional treatments.
Non-Surgical Alternatives to Eardrum Repair
While eardrum repair surgery is often the most effective solution for significant eardrum damage, there are non-surgical alternatives for minor perforations or less severe cases of eardrum injury.
Eardrum Patching: In cases of small perforations, eardrum patching may be used. This involves placing a small patch over the hole in the eardrum, allowing it to heal naturally. This procedure is typically done in an office setting with local anesthesia.
Antibiotics and Steroid Drops: For cases where chronic ear infections are present, doctors may prescribe antibiotics and steroid ear drops to reduce inflammation and prevent infection, which can help the eardrum heal on its own.
Non-invasive Hearing Aids: If hearing loss persists after a perforated eardrum has healed, hearing aids can be used to improve hearing function without the need for surgery.
While these methods can be effective in certain situations, they are typically less reliable for larger perforations or damage that extends into the middle ear. If non-surgical methods do not fully restore hearing or prevent further issues, eardrum surgery may ultimately be necessary.
Long-Term Outcomes of Eardrum Repair Surgery
Eardrum repair surgery (tympanoplasty) generally has excellent long-term outcomes, especially for patients who follow post-operative care instructions and attend follow-up appointments. The goal of the surgery is to restore hearing, prevent recurring infections, and improve ear function. Here’s what patients can expect long-term:
Hearing Restoration: Most patients experience improved hearing following eardrum repair surgery. The success rate of tympanoplasty is high, with many patients reporting a noticeable increase in hearing clarity and less muffling.
Reduced Risk of Infections: One of the main benefits of repairing the eardrum is the prevention of chronic ear infections. By sealing the perforation, the ear is better able to maintain normal pressure and fluid balance, reducing the likelihood of recurrent infections.
Enhanced Quality of Life: For many patients, hearing restoration and the prevention of ear infections lead to a significant improvement in overall quality of life. This includes better communication, reduced social isolation, and a more comfortable daily experience.
However, in some cases, there may be complications, such as graft failure or recurrent perforation, which may require further treatment. Long-term care includes regular monitoring of ear health, especially for patients with a history of ear infections or eardrum tears.
Overall, the long-term outcomes of eardrum repair surgery are positive for most individuals, with a high success rate in restoring hearing and improving ear health, ultimately enhancing the patient’s overall well-being.
Eardrum Repair Surgery Cost
The cost of eardrum repair surgery can vary depending on the country, clinic, and complexity of the procedure. In general, tympanoplasty costs between $1,500 and $4,000 in the United States. In countries like Korea, the cost is often lower, offering high-quality care at a fraction of the price, which has made it a popular destination for medical tourism.
The cost can also depend on factors like the type of anesthesia used, whether additional procedures are required (e.g., repair of the middle ear bones), and follow-up care. Some clinics in Korea offer all-inclusive packages that cover the procedure, aftercare, and even travel expenses for international patients, making it an attractive option for those seeking affordable, world-class care.
Non-Surgical Alternatives to Eardrum Repair
For minor eardrum perforations or early-stage damage, non-surgical treatments may be an option. These include:
Eardrum Patching: A non-invasive procedure where a small patch is applied to a perforation, encouraging natural healing. This is suitable for small holes and can often be done in the office under local anesthesia.
Antibiotics and Steroid Drops: For infections or inflammation causing the perforation, doctors may prescribe antibiotic and steroid ear drops to reduce inflammation and prevent infection, allowing the eardrum to heal on its own.
Hearing Aids: If hearing loss persists after an injury, hearing aids can provide significant improvement without the need for surgery.
While these methods can be effective for smaller issues, eardrum repair surgery is typically necessary for larger or more persistent perforations.
Long-Term Outcomes of Eardrum Repair Surgery
Eardrum repair surgery generally offers excellent long-term outcomes, with the majority of patients experiencing significant improvement in hearing and overall ear health. Key benefits include:
Improved Hearing: After tympanoplasty, most patients experience restored or significantly improved hearing, with a high success rate in sealing the perforation.
Reduced Infection Risk: By repairing the eardrum, patients are less likely to experience chronic ear infections.
Better Quality of Life: With restored hearing and fewer ear problems, patients often see improvements in communication and social interaction.
However, there can be some risk of recurrence, especially if post-surgical care is not followed. Regular check-ups and ear care are essential for long-term success.
Eardrum Repair Surgery in Korea
Korea is a leading destination for eardrum repair surgery, attracting international patients due to its affordable yet high-quality medical care. Korean hospitals offer advanced surgical techniques and specialized otolaryngologists skilled in performing tympanoplasty.
With cutting-edge medical technology, Korea provides not only cost-effective solutions but also outstanding patient outcomes. Many clinics cater specifically to international patients, offering comprehensive packages that include surgery, aftercare, and travel arrangements, making it an ideal option for those seeking top-tier care abroad.
In Korea, eardrum repair procedures are designed to maximize healing and restore hearing, with follow-up care to ensure the best long-term results.
Best Hospitals for Eardrum Repair in Korea
Korea is home to some of the most renowned hospitals and clinics offering eardrum repair surgery. These facilities are equipped with the latest technology and staffed by highly skilled otolaryngologists (ENT specialists). Here are some top hospitals in Korea for tympanoplasty and ear surgery:
Severance Hospital (Yonsei University Health System): Known for its state-of-the-art equipment and expert surgeons specializing in middle ear surgery and hearing restoration.
Samsung Medical Center: One of Korea’s leading medical institutions, offering advanced eardrum repair procedures and comprehensive post-surgery care.
Asan Medical Center: Renowned for its high success rates in eardrum surgery and its commitment to patient care, especially for international patients.
These hospitals offer exceptional surgical outcomes, making Korea a popular destination for eardrum repair surgery, particularly for those seeking affordable yet high-quality care.
How Eardrum Surgery Restores Hearing Volume
One of the primary goals of eardrum repair surgery is to restore hearing by fixing a perforated or damaged eardrum. When the eardrum is compromised, it affects its ability to vibrate properly, resulting in diminished hearing. By repairing the hole or tear in the eardrum, the surgery helps to restore its normal function.
Tympanoplasty repairs the eardrum with a tissue graft or other materials, sealing the perforation and enabling the eardrum to vibrate properly again. This restoration improves sound transmission from the outer ear to the inner ear, which is essential for hearing.
As a result, patients often experience a significant improvement in hearing volume and clarity after surgery, particularly for those whose hearing loss was caused by a perforated eardrum. The procedure also helps reduce the risk of future infections and further damage.
Recovery After Eardrum Surgery and Hearing Restoration
The recovery process after eardrum repair surgery varies, but most patients can expect a relatively straightforward healing timeline. The initial recovery phase typically lasts 1-2 weeks, during which patients may experience some mild discomfort, swelling, or a feeling of fullness in the ear. Pain management with prescribed medication is typically sufficient to address any discomfort.
Full recovery from tympanoplasty can take up to 1-3 months, depending on the complexity of the surgery and the individual’s healing process. During this time, it’s crucial to avoid water exposure, strenuous activities, and loud noises, which can hinder healing. Follow-up visits will ensure that the eardrum repair is healing as expected.
After the healing period, most patients notice a significant improvement in hearing and can return to their normal activities with restored ear function.
Frequently Asked Questions (FAQs)
What is the success rate of eardrum repair surgery?
The success rate of tympanoplasty is high, typically ranging from 85% to 95%, with most patients experiencing significant hearing restoration.
How long does recovery take after eardrum surgery?
Initial recovery takes about 1-2 weeks, but full recovery can take 1-3 months, depending on the extent of the surgery and individual healing.
Are there risks involved in eardrum surgery?
As with any surgery, there are risks, including infection, bleeding, or graft failure. However, these risks are minimized with careful surgical planning and proper aftercare.
Is eardrum repair surgery covered by insurance?
Coverage for eardrum repair surgery varies by insurance provider and country. It is recommended to check with your insurance company for specific details regarding coverage for tympanoplasty.
Can eardrum repair surgery be done in Korea?
Yes, eardrum repair surgery is widely available in Korea at leading hospitals with advanced medical technology and skilled specialists.
These FAQs aim to address common concerns about eardrum repair surgery and offer helpful information for those considering the procedure.
Conclusion
Eardrum repair surgery, or tympanoplasty, is an effective solution for restoring hearing and preventing further complications caused by eardrum damage. Whether the damage is due to trauma, chronic ear infections, or perforation, this procedure offers significant benefits in improving ear function, preventing recurring infections, and ultimately restoring hearing.
With a high success rate and the ability to repair damage to both the eardrum and middle ear bones, eardrum repair surgery provides a lasting solution to hearing loss and ear discomfort. Recovery is typically straightforward, with most patients experiencing noticeable improvements in hearing and quality of life.
For those considering surgery, especially international patients, Korea has become a leading destination for eardrum repair procedures, offering advanced medical care at affordable prices. With top hospitals and highly skilled surgeons, Korea provides exceptional options for individuals seeking safe and effective hearing restoration.
If you are dealing with eardrum damage or persistent ear issues, consulting with a qualified ENT specialist can help determine the best course of treatment and ensure optimal outcomes from your surgery.