Introduction
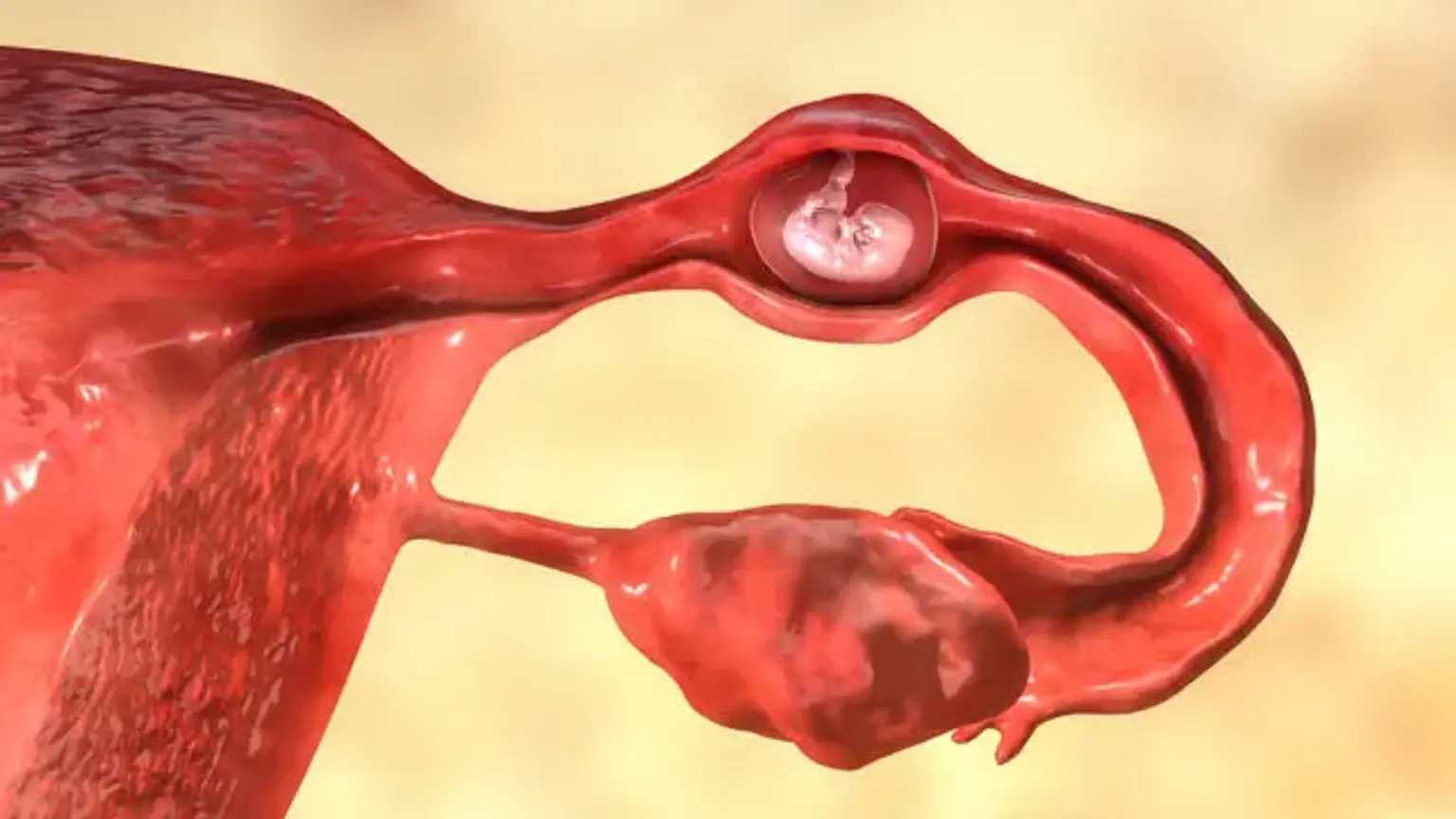
Unilateral fallopian tube removal, or salpingectomy, is a surgical procedure where one of the fallopian tubes is removed. This procedure is typically performed to treat specific health conditions, such as ectopic pregnancies, severe infections, or cancer affecting the fallopian tube. While it may sound daunting, many women who undergo unilateral fallopian tube removal continue to have successful pregnancies, as the remaining fallopian tube can often compensate for the loss of the other.
In this article, we’ll explore why and how the procedure is performed, what patients can expect during and after surgery, and the potential effects on fertility.
Indications for Unilateral Fallopian Tube Removal
Several medical conditions may necessitate the removal of one fallopian tube. These include:
Ectopic pregnancy: If a pregnancy implants in a fallopian tube, it can cause life-threatening complications. In such cases, removing the affected tube may be necessary to protect the woman’s health.
Severe infections: Chronic infections like pelvic inflammatory disease (PID) can damage the fallopian tubes, leading to scarring and blockage. If conservative treatments fail, a tube may need to be removed.
Tubal disease: Conditions like endometriosis can cause tubes to become blocked or damaged, impacting fertility.
Cancer: Cancerous growths in the fallopian tube, though rare, may require surgical removal to prevent the spread of the disease.
For women facing these conditions, unilateral fallopian tube removal can significantly improve their overall health and prevent further complications.
How Unilateral Fallopian Tube Removal is Performed
Unilateral fallopian tube removal is generally done using laparoscopic surgery, a minimally invasive technique that uses small incisions and a camera to guide the surgeon. This method typically requires fewer risks and results in a faster recovery compared to open surgery.
Here’s how the procedure typically goes:
Anesthesia: The patient is given general anesthesia to ensure they are asleep during the surgery.
Incisions: A small incision is made near the belly button, and a laparoscope (a thin tube with a camera) is inserted to visualize the organs.
Removal: The surgeon removes the damaged fallopian tube through another small incision.
Closure: The incisions are closed with stitches, and the patient is taken to recovery.
The entire procedure usually takes around 30 to 60 minutes, depending on the complexity of the surgery. In some cases, the surgery can be done on an outpatient basis, meaning the patient can return home the same day.
What is Unilateral Fallopian Tube Removal?
Unilateral fallopian tube removal is the surgical removal of one fallopian tube, usually because it has become damaged or diseased. The fallopian tubes are essential for transporting eggs from the ovaries to the uterus, and a healthy fallopian tube is crucial for fertility. However, if one tube becomes blocked or damaged, it may no longer function effectively, leading to fertility challenges or other health concerns.
This surgery is typically performed when:
Ectopic pregnancy occurs, where the fertilized egg implants outside the uterus, often in a fallopian tube.
Infection such as pelvic inflammatory disease (PID) severely damages the tube.
Cancer affects the fallopian tube.
Tubal blockage or endometriosis impacts the tube’s function.
What to Expect During the Surgery
Unilateral fallopian tube removal is typically a straightforward procedure, especially when performed laparoscopically. Here's what patients can expect during the surgery:
Pre-surgery: Before the procedure, you'll be asked to refrain from eating or drinking for several hours. A pre-surgical assessment, including blood tests, may be done to ensure you're fit for surgery.
Anesthesia: The procedure is done under general anesthesia, meaning you'll be asleep throughout the surgery. Anesthesia is carefully monitored to ensure safety.
Surgical Process: The surgeon will make small incisions in your abdomen, through which they will insert a laparoscope and other surgical instruments. Using a camera, they will locate and remove the affected fallopian tube.
Post-surgery: After the surgery, you'll be monitored in a recovery room until the anesthesia wears off. Most patients are discharged the same day, although a short hospital stay may be required if complications arise.
The surgery typically lasts between 30-60 minutes. It’s minimally invasive, which leads to a faster recovery compared to traditional open surgery.
Safety Protocols and Best Practices
Ensuring safety during unilateral fallopian tube removal is critical. Here are some best practices:
Qualified Surgeons: Choose a board-certified gynecologist or reproductive surgeon with experience in laparoscopic procedures. Their expertise helps reduce risks during surgery.
Pre-surgical Screening: A thorough medical evaluation, including blood tests and imaging, is essential to assess your overall health and to ensure the procedure is the right choice.
Sterile Technique: During the surgery, your surgical team will use strict sterile techniques to minimize infection risk. The surgical area will be disinfected, and only sterile instruments will be used.
Post-op Monitoring: After surgery, your recovery will be monitored to catch any early signs of complications, such as bleeding or infection. You’ll be given clear instructions on how to care for the surgical site at home.
Following the surgeon’s advice and attending follow-up appointments is key to ensuring a smooth and safe recovery.
Risks and Potential Complications
As with any surgery, unilateral fallopian tube removal carries some risks. While complications are rare, it's important to be aware of them:
Infection: Any surgery carries a risk of infection, but this is minimized by following proper sterilization techniques and post-surgical care instructions.
Bleeding: Although uncommon, excessive bleeding can occur. This is usually managed during surgery, but in rare cases, additional interventions may be needed.
Damage to Nearby Organs: During the surgery, there is a small risk of damaging other organs, such as the ovaries or bladder. However, laparoscopic surgery is precise, and the risk is minimal.
Adhesions: Scar tissue (adhesions) can form after surgery and may affect fertility in some cases. Your surgeon will aim to minimize this risk, but it can occur.
Emotional Effects: While not a physical complication, some women may experience emotional challenges, especially if the surgery impacts fertility or if the procedure is performed due to a miscarriage or cancer diagnosis. It's important to discuss any concerns with your healthcare provider.
Discussing potential risks with your surgeon before the surgery can help set realistic expectations and prepare you for a smooth recovery.
Psychological and Emotional Impact of the Procedure
Undergoing unilateral fallopian tube removal can have emotional and psychological effects, particularly if the surgery was performed due to infertility or an ectopic pregnancy. Here’s what patients may experience:
Emotional Response: It’s common to feel a sense of loss, especially if the procedure was done because of fertility issues or an ectopic pregnancy. For some women, the thought of having one less fallopian tube can raise concerns about future pregnancies.
Coping Mechanisms: It's important to allow yourself time to grieve if necessary. Counseling or speaking with a therapist can help process any emotional distress related to fertility or body image changes.
Support: Talking to your doctor about expectations and recovery, as well as seeking support from loved ones or support groups, can make a significant difference in your emotional well-being during recovery.
Understanding that the remaining fallopian tube can often compensate for the lost one helps many women regain confidence in their ability to conceive.
Effect of Unilateral Fallopian Tube Removal on Fertility
One of the most common concerns following unilateral fallopian tube removal is its impact on fertility. Here’s what you should know:
Can you still get pregnant with one fallopian tube? Yes! Women with only one functioning fallopian tube can still get pregnant. The remaining tube often compensates for the loss of the other. However, fertility may be slightly reduced because there is only one tube to transport eggs.
Improved Chances of Conception: In many cases, women with a single fallopian tube can conceive naturally. The other tube often becomes more efficient at transporting eggs and capturing sperm.
Assisted Reproductive Technology (ART): If pregnancy does not occur naturally, assisted reproductive techniques like in vitro fertilization (IVF) can help. In IVF, eggs are harvested directly from the ovaries, bypassing the fallopian tubes.
Health of the Remaining Tube: The fertility outcome largely depends on the health of the remaining fallopian tube and whether it is functioning well. Women with a healthy tube typically experience good fertility outcomes after surgery.
Time to Conception: For those trying to conceive after unilateral fallopian tube removal, it may take a bit longer than before, but most women do conceive naturally within a year. It’s important to consult with a fertility specialist if pregnancy doesn’t occur after several months of trying.
Ultimately, the removal of one fallopian tube does not mean the end of fertility for many women. With proper care and monitoring, they can go on to have successful pregnancies.
Effect on Ovarian Function and Hormonal Balance
The removal of one fallopian tube does not typically affect ovarian function or hormonal balance. The ovaries remain intact, continuing to produce eggs and hormones like estrogen and progesterone. These hormones regulate your menstrual cycle and support fertility.
Ovarian Function: As long as the ovaries are healthy, they will continue to release eggs each month. The remaining fallopian tube often adjusts to capture the eggs released from the ovary on the side of the surgery.
Hormonal Balance: Since the ovaries are responsible for hormone production, removing a fallopian tube won’t interfere with the hormonal cycles or menstruation. Women will continue to have regular periods unless other underlying conditions exist.
However, if the removed tube was involved in disease, such as endometriosis, that condition may have affected ovarian function, which should be evaluated separately.
Recovery and Aftercare
Recovery after unilateral fallopian tube removal is relatively quick, thanks to the minimally invasive laparoscopic technique. Here’s what you can expect in terms of recovery:
Immediate Recovery: You may feel groggy and experience some pain or discomfort after the surgery, but this is usually manageable with prescribed pain medication. Some bloating or shoulder pain (due to gas used in laparoscopic surgery) may occur but should subside within a few days.
Hospital Stay: In most cases, patients can go home the same day. However, you may be kept overnight if you had a more complicated surgery or if you're experiencing significant pain.
Activity Restrictions: For the first few days, you'll need to rest and avoid heavy lifting or strenuous activity. Your doctor will advise when it’s safe to resume normal activities. Most women can return to work within a week, but avoid high-impact exercise for about 4 to 6 weeks.
Follow-up Care: You will have a follow-up appointment with your doctor within a few weeks to ensure proper healing and to address any concerns. This is also a chance to discuss fertility and any further treatment, if needed.
Most women recover fully within 1 to 2 weeks and can resume their normal routine, although some may experience mild discomfort for up to a month.
Preparing for Unilateral Fallopian Tube Surgery
Proper preparation is important for a successful surgery and smooth recovery. Here's how to get ready:
Medical Evaluation: Before surgery, your doctor will conduct a thorough evaluation, including medical history review and possibly imaging tests (like an ultrasound) to assess the condition of your fallopian tubes and ovaries.
Pre-Surgery Instructions: You’ll be instructed to avoid eating or drinking for several hours before the procedure. You may also need to stop taking certain medications, especially blood thinners, to reduce the risk of bleeding.
Arranging Support: Since you may be groggy post-surgery, arrange for someone to drive you home and assist you during the first 24 hours.
Mental Preparation: Understanding the procedure, potential risks, and what to expect can help reduce anxiety. It’s a good idea to write down any questions for your doctor beforehand to ensure you feel fully prepared.
Good preparation can help you feel more in control and reduce any worries about the procedure.
Long-Term Effects and Outlook After Surgery
The long-term outlook after unilateral fallopian tube removal is generally positive, especially if the surgery was performed to address an infection or ectopic pregnancy. Most women recover well and can return to their normal routine. However, there are a few considerations to keep in mind for the future:
Fertility: Many women with one fallopian tube go on to conceive naturally. The remaining tube often compensates for the loss of the other, although fertility may take a bit longer to achieve. If conception doesn’t happen naturally after a year of trying, consulting with a fertility specialist is a good next step.
Health Monitoring: After surgery, it's important to continue regular gynecological exams to monitor reproductive health. In some cases, if the underlying condition (like endometriosis or infection) persists, further treatment may be required.
Pregnancy: For women who have had an ectopic pregnancy or infection, the risk of future complications (like another ectopic pregnancy) is higher. It’s crucial to seek immediate medical care if you suspect any unusual symptoms in a future pregnancy.
With the right care, most women with one fallopian tube can lead a normal, healthy life and maintain their fertility.
Cost and Insurance Coverage
The cost of unilateral fallopian tube removal can vary based on several factors, including location, type of surgery (laparoscopic vs. open), and whether it's done in a private or public hospital. On average, the cost can range from $5,000 to $15,000, including pre-surgery consultations, anesthesia, and hospital fees.
Insurance Coverage: Many health insurance plans cover the cost of the surgery if it is deemed medically necessary. This includes cases of ectopic pregnancy, infections, or cancer. However, if the surgery is performed for elective reasons, such as to address fertility concerns, insurance coverage may be limited.
Out-of-Pocket Costs: Patients may have out-of-pocket expenses for certain aspects of the procedure, such as post-surgery medications, consultations, and follow-up visits. It’s important to check with your insurance provider and hospital for an estimate of costs before scheduling the surgery.
For those struggling with the costs, some clinics offer financing options or payment plans.
Alternative Treatments and Procedures
For those who experience fertility issues after unilateral fallopian tube removal, there are alternative treatments available:
In Vitro Fertilization (IVF): IVF is an option for women who struggle to conceive with one fallopian tube. It bypasses the need for a functioning tube by fertilizing eggs outside the body and then implanting the embryo into the uterus.
Ovulation Induction: For women with irregular cycles or ovulation issues, medications can stimulate the ovaries to release eggs, increasing the chances of conception, even with one tube.
Surgical Alternatives: In some cases, if there’s damage to both tubes, tubal reversal surgery might be considered, though its success rate can vary based on individual circumstances.
Consulting with a fertility specialist is essential for determining the most appropriate treatment based on individual health and fertility goals.
Frequently Asked Questions (FAQs)
1. Can I still get pregnant with one fallopian tube?
Yes, many women with one healthy fallopian tube can still get pregnant. The remaining tube can often handle the job of transporting eggs, although it may take slightly longer for conception to occur.
2. How soon can I get pregnant after surgery?
After surgery, it's advised to wait a few months before trying to conceive to allow your body time to heal. However, many women are able to conceive naturally within a year of the procedure.
3. Are there any permanent side effects of having one fallopian tube?
Most women recover without any long-term issues. However, some may experience a reduced chance of pregnancy, particularly if there are other fertility challenges. It’s important to monitor reproductive health regularly with your doctor.
4. Will my periods change after the surgery?
No, since the ovaries are not affected by the removal of the fallopian tube, your menstrual cycle should remain normal. However, if the surgery was performed due to a condition like endometriosis, menstrual changes may be more likely.
5. What are the risks of the surgery?
As with any surgery, risks include infection, bleeding, and damage to surrounding organs. However, these risks are minimized with proper preparation and surgical technique.
The Role of Diet and Lifestyle in Recovery
A healthy lifestyle and diet can significantly impact your recovery after unilateral fallopian tube removal. Here are some tips for supporting your body during recovery:
Eat a Balanced Diet: Eating nutrient-rich foods supports your body’s healing process. Include protein, healthy fats, and plenty of fruits and vegetables. Iron-rich foods can help prevent anemia, especially if you experience mild blood loss during surgery.
Stay Hydrated: Drink plenty of fluids to stay hydrated, which aids in the recovery process and helps prevent complications like constipation from pain medications.
Exercise: After getting clearance from your doctor, light physical activity, like walking, can improve circulation and promote healing. Avoid strenuous exercise until you’re fully recovered.
Manage Stress: Stress can hinder recovery, so take time to relax and practice mindfulness or meditation. Ensure you get enough sleep to support your body’s healing process.
Support Systems and Resources
Dealing with the aftermath of unilateral fallopian tube removal can be challenging, both physically and emotionally. Here are some support resources:
Support Groups: Online communities and in-person groups offer emotional support for women who have undergone similar surgeries. Sharing experiences can help you feel less isolated and provide valuable insights.
Counseling: Talking to a therapist or counselor can be beneficial, especially for those who may struggle with fertility issues or emotional recovery after surgery.
Family and Friends: Having a support system at home can make a huge difference. Don’t hesitate to reach out for help during your recovery, whether it's for practical support or emotional encouragement.
It’s important to remember that you're not alone, and seeking help when needed is key to navigating this journey.
Conclusion
Unilateral fallopian tube removal, while a significant procedure, is often a necessary step in preserving long-term health and fertility. With proper care, most women experience a smooth recovery and can go on to conceive naturally or with assisted reproductive technologies.
By understanding the procedure, preparing for recovery, and seeking emotional support, you can navigate this process with confidence. Whether you're concerned about fertility or managing post-surgery changes, working closely with your healthcare provider is crucial to achieving the best outcome.
Remember, having one fallopian tube doesn’t mean the end of your fertility journey. With the right care and support, you can continue to lead a healthy life and pursue your reproductive goals.