Cholelithiasis
Overview
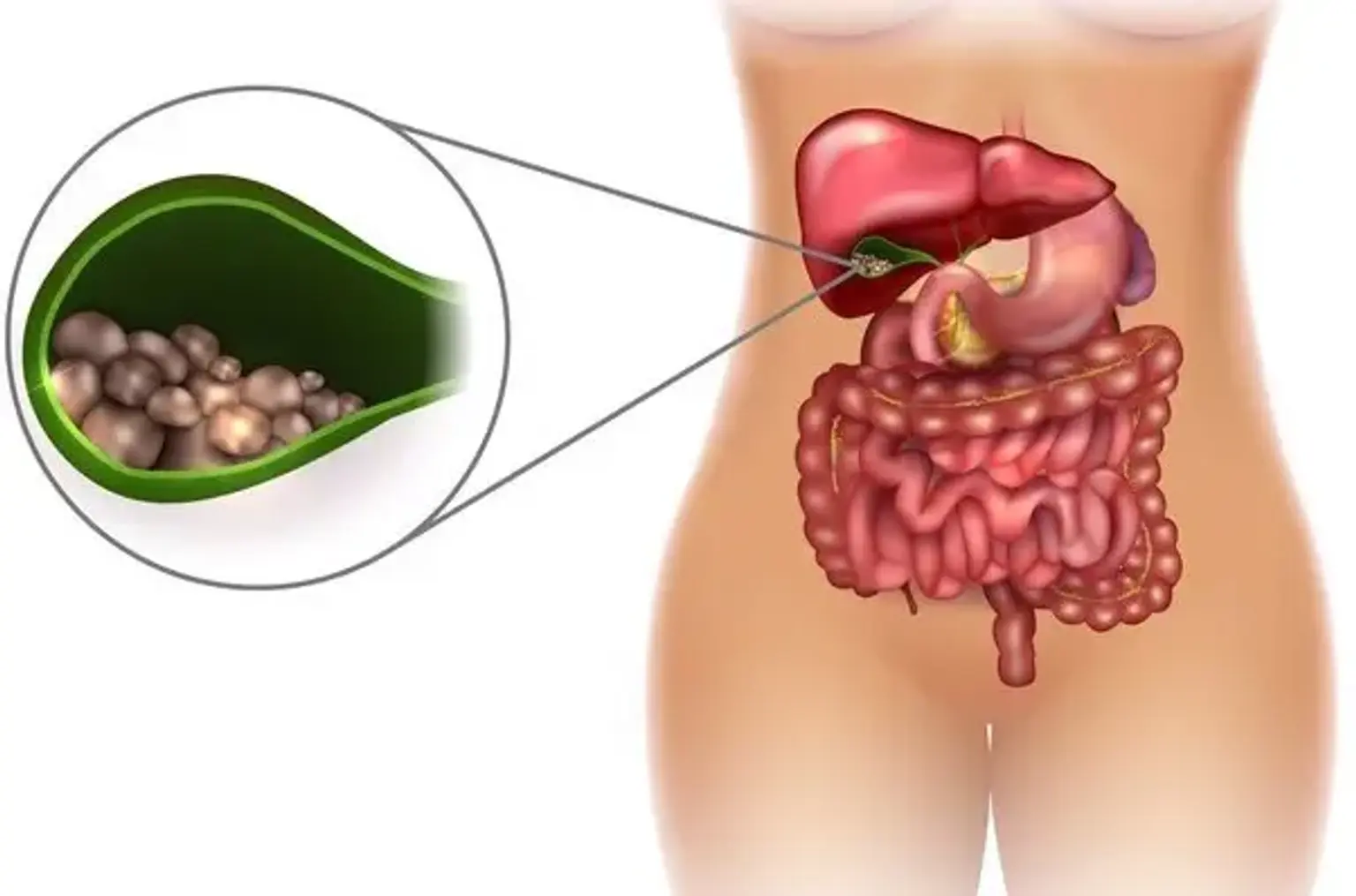
Gallstones, also known as cholelithiasis, are hardened deposits of digestive fluid that can form in your gallbladder. The gallbladder is a tiny organ found directly below the liver. The gallbladder stores bile, a digestive fluid that is discharged into the small intestine. Gallstones affect 6% of men and 9% of women in the United States, with the majority of cases being asymptomatic. The chance of developing symptoms or consequences in persons with asymptomatic gallstones identified inadvertently is 1% to 2% every year.
Asymptomatic gallbladder stones discovered in a healthy gallbladder and biliary tree do not require treatment unless they cause symptoms. However, after 15 years of follow-up, roughly 20% of these asymptomatic gallstones will develop symptoms. Complications from gallstones include cholecystitis, cholangitis, choledocholithiasis, gallstone pancreatitis, and, in rare cases, cholangiocarcinoma.
What is Cholelithiasis?
Gallstones, also known as cholelithiasis, are hardened deposits of digestive fluid that accumulate in the gallbladder. The gallbladder is a tiny, pear-shaped organ located under the liver that stores bile produced by the liver. Bile is a digestive fluid composed of cholesterol, bile salts, and bilirubin that enters the small intestine via the cystic and common bile ducts to help in fat breakdown. Gallstones vary in size, and an individual may acquire multiple little gallstones, one giant gallstone, or a mix of gallstones of various sizes. In the United States, around 6% of men and 9% of women develop cholelithiasis, the majority of whom have no symptoms.
Cholelithiasis is fairly prevalent, affecting around 6% of men and 9% of women. Native American populations had the greatest rate of cholelithiasis. Gallstones are uncommon in Africa and Asia. The obesity pandemic has most certainly exacerbated the rise of gallstones.
Regardless matter how common gallstones are, more than 80% of patients are asymptomatic. Biliary discomfort, on the other hand, will develop in 1% to 2% of previously asymptomatic persons each year. Major problems (cholecystitis, choledocholithiasis, gallstone pancreatitis, cholangitis) occur at a rate of 0.1% to 0.3% annually in those who began to develop symptoms.
What causes cholelithiasis?
There are three main pathways in the formation of gallstones:
- Cholesterol supersaturation: Bile can normally dissolve the quantity of cholesterol released by the liver. However, if the liver generates more cholesterol than bile can breakdown, the extra cholesterol may crystallize. Gallbladder sludge is formed when crystals become caught in gallbladder mucus. With time, the crystals may expand to form stones and obstruct the ducts, resulting in gallstone disease.
- Excess bilirubin: Liver cells release bilirubin, a yellow pigment resulting from the breakdown of red blood cells. Certain hematologic disorders lead the liver to produce an excessive amount of bilirubin during the breakdown of hemoglobin. Excess bilirubin may also result in gallstone development.
- Gallbladder hypomotility or reduced contractility: Bile can get concentrated and produce gallstones if the gallbladder does not drain properly.
Gallstones are composed differently depending on their cause. Cholesterol gallstones, black pigment gallstones, and brown pigment gallstones are the three most prevalent forms. Gallstones made up of cholesterol account for 90% of all cases.
Each stone has its own set of dangers. Obesity, age, female gender, pregnancy, heredity, complete parenteral feeding, fast weight loss, and certain drugs are all risk factors for the formation of cholesterol gallstones (oral contraceptives, clofibrate, and somatostatin analogs).
Black and brown pigment stones account for around 2% of all gallstones. These can be detected in people who have a high hemoglobin turnover. The pigment is largely made up of bilirubin. Black pigment stones are common in patients with cirrhosis, ileal disorders, sickle cell anemia, and cystic fibrosis. Brown pigments are mostly present among Southeast Asians and are uncommon in the United States. Intraductal stasis and persistent bile bacterial colonization are risk factors for brown pigment stones.
The most important risk factors for the development of gallstones are:
- Overweight
- The female sex
- Age over 40 years old
- Pregnancy
- European, Native American, or Hispanic descent
- Family members with gallstones
- Certain medications
- Some pre-existing conditions – such as diabetes, sickle cell anemia, cirrhosis of the liver, cystic fibrosis, and Crohn's disease
How do gallstones form?
Cholesterol gallstones arise primarily as a result of excessive cholesterol release by liver cells and hypomotility or delayed gallbladder emptying. Bilirubin concentrations in bile may be greater than usual in pigmented gallstones due to excessive heme turnover. Bilirubin can then crystallize and create stones.
Cholelithiasis symptoms and problems occur when stones restrict the cystic duct, bile ducts, or both. Temporary obstruction of the cystic duct (as when a stone lodges in the duct before dilation and the stone returns to the gallbladder) causes biliary pain but is usually temporary. This is referred to as cholelithiasis. More prolonged cystic duct blockage (as when a big stone becomes permanently lodged in the neck of the gallbladder) might result in acute cholecystitis. A gallstone can pass through the cystic duct and get stuck and impacted in the common bile duct, causing blockage and jaundice. Choledocholithiasis is the medical term for this problem.
If gallstones travel through the cystic duct, common bile duct, and get dislodged at the ampulla of the distal segment of the bile duct, acute gallstone pancreatitis can occur due to fluid backup and increased pressure in pancreatic ducts, as well as in situ activation of pancreatic enzymes. Large gallstones can perforate the gallbladder wall and form a fistula between the gallbladder and the small or large bowel, resulting in intestinal blockage or ileus.
What are the signs and symptoms of cholelithiasis?
Gallstone disease is characterized by biliary colic symptoms (intermittent bouts of continuous, acute right upper quadrant (RUQ) stomach pain, frequently accompanied by nausea and vomiting), normal physical examination findings, and normal laboratory test results. Diaphoresis, nausea, and vomiting are possible side effects.
- Biliary colic is often produced by the gallbladder constricting in response to some sort of stimulation, driving a stone through the gallbladder into the cystic duct opening, resulting in increased gallbladder wall tension and pressure, which frequently results in discomfort. The stones frequently slide back into the gallbladder when the gallbladder relaxes, and the discomfort usually goes away within 30 to 90 minutes.
- Fatty foods are a frequent cause of gallbladder constriction. The discomfort generally begins an hour after a fatty meal and is reported as strong and dull, lasting 1 to 5 hours. However, the relationship with meals is not ubiquitous, and a considerable number of individuals have discomfort at night. The frequency of recurring episodes varies, although most individuals do not have symptoms on a daily basis.
- A comprehensive physical exam can help differentiate between biliary discomfort caused by acute cholecystitis, simple cholelithiasis, and other problems.
- The patient is afebrile and has a basically benign abdominal examination with no rebound or guarding in simple biliary colic.
When a persistent stone dislodges the cystic duct, it causes the gallbladder to become bloated and inflamed. Fever, discomfort in the right upper quadrant, and soreness above the gallbladder may also be present (this is known as Murphy's sign).
When fever, prolonged tachycardia, hypotension, or jaundice are present, it is necessary to look for cholelithiasis complications such as cholecystitis, cholangitis, pancreatitis, or other systemic causes.
Gallstones that pass through the cystic duct and clog the common bile duct can cause choledocholithiasis, which is characterized by itchy skin and/or skin and eye yellowing, often known as jaundice. Persistent bile duct obstruction can cause pancreatitis or a major infection, which is characterized by high temperature, sweating, chills, fast pulse, nausea, vomiting, and diarrhea.
Cholangitis is caused by bacterial colonization and overgrowth in stagnant bile above an obstructing common duct stone. Purulent inflammation of the liver and biliary tree results. Charcot's triad is characterized by significant RUQ discomfort, fever, and jaundice, and is typical with cholangitis. To treat this disease, surgical removal of the stone blockage along with intravenous antibiotics is necessary.
How is cholelithiasis diagnosed?
CBC, CMP, PT/PTT, lipase, amylase, Alk Phos, total bilirubin, and urine tests are frequently used to assess gallstones.
Ultrasound is still the best imaging technique for diagnosing gallstones. According to a comprehensive study, the sensitivity was 84% and the specificity was 99%, which was higher than for other modalities. Biliary disease can be detected using either a radiology ultrasound scan or a point-of-care ultrasound. Several studies in the literature have indicated that doctors' use of point-of-care ultrasonography to diagnose or rule out biliary illness is accurate and trustworthy.
Gallstones emerge as hyperechoic entities inside the gallbladder with distal acoustic shadowing on ultrasonography. Sludge in the gallbladder may be observed, as well as hyperechoic layers within the gallbladder. Unlike stones, sludge does not cast acoustic shadows. Additional symptoms of acute cholecystitis include a thicker anterior gallbladder wall (more than 3 mm), the presence of pericholecystic fluid, and a positive sonographic Murphy's sign.
Ultrasound can be used to get common bile duct (CBD) measures, which, if elevated, can indicate choledocholithiasis. In patients under the age of 40, the usual CBD range is four millimeters, with a further one millimeter permitted for each consecutive decade of life. Because the common duct becomes the bile reservoir after the gallbladder is removed, post-Cholecystectomy patients are permitted up to 10 mm diameter.
A nuclear medicine cholescintigraphy scan, commonly known as a HIDA scan, can be conducted if an ultrasound examination is inconclusive in ruling out acute cholecystitis. A radioactive tracer injected into a peripheral vein is transported to the liver, where it enters the biliary network and is taken up by the gallbladder within 4 hours in a typical healthy gallbladder. A sick gallbladder with a blocked cystic duct prevents the tracer from accessing the gallbladder. For the diagnosis of acute cholecystitis, the HIDA scan has a sensitivity of up to 97% and a specificity of 94%.
Abdominal CT imaging does not improve sensitivity or specificity in identifying gallstones or cholecystitis. It can identify pancreatic inflammation or problems and determine if CBD dilatation is present (masses, pseudo-cysts, necrotizing features). If RUQ ultrasound excludes biliary illness and alternative reasons of stomach discomfort are being explored, CT imaging might be helpful.
Endoscopic retrograde cholangiopancreatography (ERCP) is a diagnostic and therapy technique that involves inserting a long, thin, and flexible tube with a camera attached (i.e., an endoscope) through the mouth and down toward the small intestine. During an ERCP, an imaging dye is injected into the body to highlight the biliary system's ducts. The endoscope may remove gallstones from the bile ducts; however, the endoscope cannot remove stones from the gallbladder.
Magnetic resonance cholangiopancreatography (MRCP) is a diagnostic technique that uses magnetic resonance imaging to evaluate the bile ducts. This treatment produces a more comprehensive image, is less intrusive, and is a safer option for the majority of people. In severe situations (for example, ascending cholangitis), ERCP may be performed before MRCP. An endoscope is put into the mouth, down toward the common bile duct and gallbladder area, to check for gallstones that are not evident on an abdominal ultrasound. Following an MRCP or EUS, an ERCP may be performed to remove the visible gallstones from the bile ducts.
How is cholelithiasis treated?
Treatment choices for cholelithiasis are determined by the individual's age, overall health, medical history, severity of symptoms, and the size, location, and number of gallstones.
Cholelithiasis may not require treatment in asymptomatic persons. Cholelithiasis can be treated with drugs that dissolve gallstones, by specific diagnostic examinations, or through gallbladder removal surgery, also known as a cholecystectomy, in people who have symptoms. If an individual is unable to undergo an invasive operation, medications used to dissolve gallstones, such as ursodiol, may be utilized; however, this strategy is limited in efficacy, requires extended treatment durations, and has a significant chance of gallstone recurrence once the medicine is no longer taken.
Extracorporeal shockwave lithotripsy is a treatment that pulverizes gallstones using shock waves. Remnants can then pass through the bile ducts without being clogged. If the gallstones are not inside the gallbladder, ERCP is an efficient treatment for removing them from the bile ducts. Another operation that may be conducted during an ERCP is a sphincterotomy, which involves cutting tight rings of muscle around the entrances of bile ducts to enlarge the breadth of the bile ducts when open and allow gallstones to flow into the gut.
When gallstones are found inside the gallbladder, gallbladder removal surgery is often performed. A cholecystectomy removes the possibility of recurring cholelithiasis and permits bile to pass straight from the liver into the small intestine. Diarrhea may occur as a result. The most frequent cholecystectomy is a laparoscopic cholecystectomy, which is minimally invasive and includes the use of a laparoscope, or a thin tube with a camera.
To see and remove the gallbladder, a laparoscope is introduced via one of many tiny incisions in the belly. If a laparoscopic cholecystectomy fails or a person develops cholelithiasis problems, an open cholecystectomy may be performed, which includes one big incision to the abdomen and a lengthier recovery period.
When a cholecystectomy is not a viable option owing to sickness, a percutaneous drainage procedure may be performed in which a drainage tube is introduced into the gallbladder via the belly to allow for infection drainage until a cholecystectomy can be performed. Certain people may need antibiotics after a cholecystectomy, such as ciprofloxacin and metronidazole, to prevent or treat residual infection.
Does cholelithiasis require surgery?
Cholelithiasis may necessitate surgery, such as a laparoscopic or open cholecystectomy. These treatments are most typically used in those who have significant symptoms and gallstones in their gallbladder. Individuals who are asymptomatic or have gallstones elsewhere in their body, such as the bile ducts, may not need surgery.
- Laparoscopic cholecystectomy: The gallbladder is removed through a tiny incision in the abdomen during this sort of keyhole surgery.
- In some cases, a person can go home on the same day.
- In other cases, you will need to stay in the hospital for a few days of monitoring.
- Open cholecystectomy: This is an earlier form of surgery in which the gallbladder is removed through a bigger incision in the belly.
- This may be necessary if laparoscopy is not advisable or complications occur.
- The recovery time is longer with this type of surgery
Prognosis
According to data, just half of people with gallstones have symptoms. The risk of death after elective laparoscopic cholecystectomy is less than 1%. Emergency cholecystectomy, on the other hand, is linked with a significant fatality rate. Other issues include stones in the bile duct following surgery, incisional hernia, and bile duct damage. A small percentage of people have post-cholecystectomy discomfort.
Without a gallbladder, you may live a normal and healthy life. Following gallbladder removal, bile travels straight from the liver into the intestine via the connected bile duct, rather than being briefly held in the gallbladder as previously. Bile continues to aid digestion as usual. Mild diarrhea or digestive problems may develop in certain circumstances. A cholecystectomy carries a minimal risk of complications.
Cholelithiasis Complications
The vast majority of persons with gallstones have no symptoms. In most of these circumstances, no therapy is required. Even if symptoms do arise, there are now low-risk therapeutic options available, making the prognosis quite optimistic.
In individual cases, or if no treatment is given for existing complaints, the following complications may occur:
- Cholecystitis (inflammation of the gallbladder)
- Pancreatitis (inflammation of the pancreas)
- Injury and/or infection of the bile ducts (Inflammation of the bile ducts is referred to as cholangitis.)
- Intestinal obstruction.
These complications often require emergency treatment. As already mentioned above, medical attention should be sought immediately for the following symptoms:
- Severe, persistent pain in the abdomen
- Fever
- Chills
- Yellowing of the skin or eye whites (jaundice).
Conclusion
Gallstones are hard, crystal-like deposits that can develop in the gallbladder under the liver and are also known as symptomatic cholelithiasis. Pain in the upper right or central area of the abdomen, exactly below the ribs, is the most common sign of symptomatic gallstones. When a clinician gathers a person's medical history and physical examination, as well as laboratory testing and ultrasound, the diagnosis is usually determined promptly. Treatment is tailored to each unique instance. Overall, the outlook is favorable.