Complex Coronary Interventions
Overview
Chronic total occlusion (CTO) is a severe form of coronary artery disease in which the coronary arteries are completely (or nearly so) blocked by fatty deposits or plaque. Complex coronary interventions such as angioplasty and stenting can completely (or nearly completely) open clogged arteries.
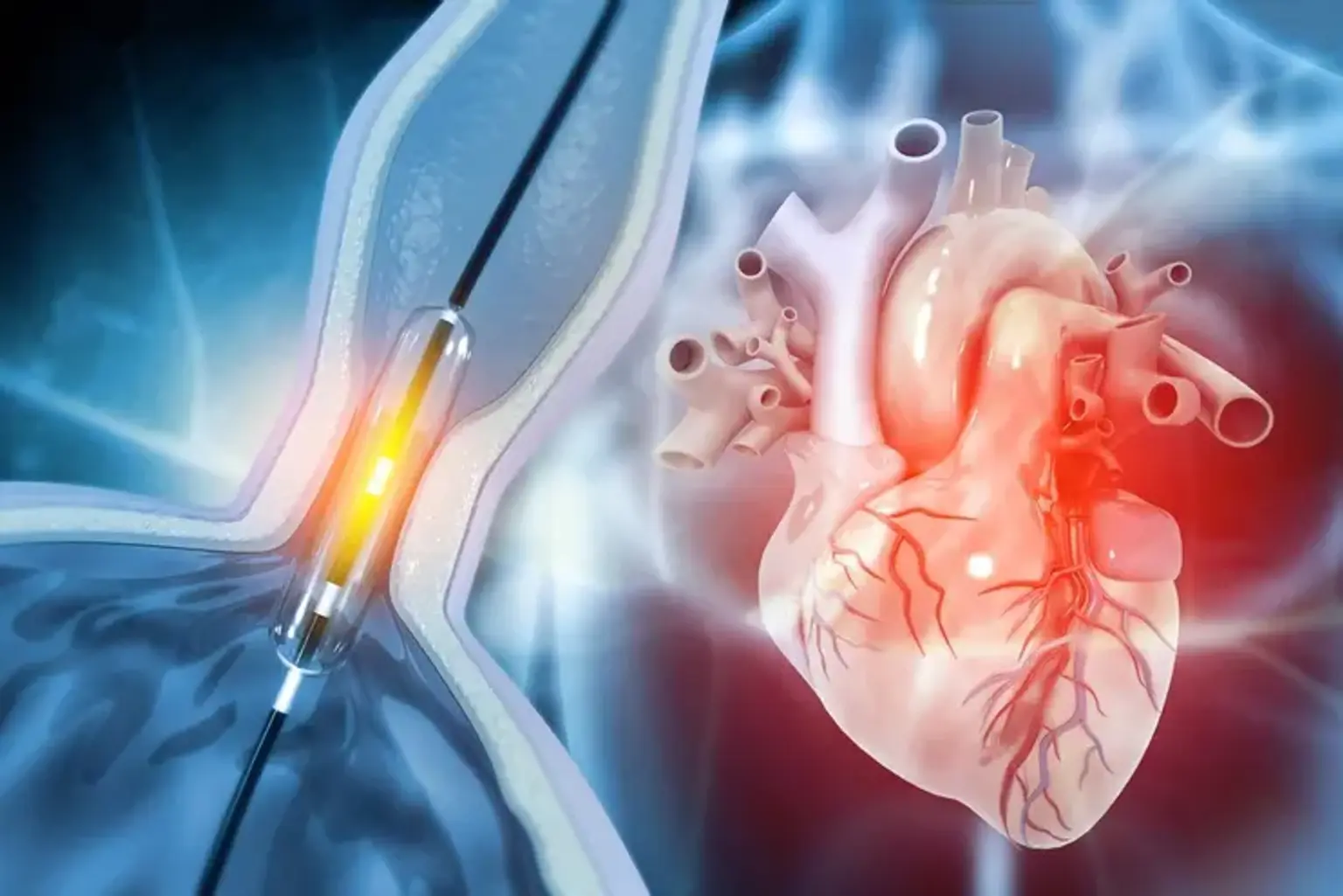
In a complex coronary intervention, a fine angioplasty catheter is inserted into the affected coronary arteries. Using advanced imaging technology, one of our physicians will carefully guide the angioplasty catheter to the narrowest part of the coronary artery.
A wire with a ballooned tip will be inserted through the catheter, widening the narrowed artery and improving blood flow. The angioplasty balloon will then be removed, and a catheter with a closed stent will be inserted. He will then insert the stent into the artery, which will push against the artery's walls, acting as a support to keep it open. This procedure is minimally invasive and will not necessitate any large incisions.
What is Chronic Total Occlusion (CTO)?
Chronic Total Occlusion (CTO) is a complete blockage of a coronary artery caused by plaque build-up that has hardened over time in the arteries.
CTO patients may experience the following symptoms:
- Normal activity causes chest pain (angina).
- Normal activity causes shortness of breath.
- Fatigue or a reduction in exercise tolerance
- Normal activity causes pain in the neck, arm, or back.
CTOs are typically treated solely with medications or with coronary artery bypass graft surgery (open heart surgery). With advances in technology and skills, it is now possible to use balloons and stents to recanalize these completely blocked arteries. Patients experience symptom relief and are able to resume their favourite activities following CTO recanalization.
How Safe is the Procedure?
The operation carries a slightly increased risk of kidney injury due to the use of intravenous contrast and bleeding at the entry site into groin arteries. Most additional dangers, however, are comparable to those observed with more normal angioplasty and can include:
- Bleeding at the location of the puncture.
- Blood vessel damage at the puncture location.
- The coronary artery suddenly closes.
- A small tear in the artery's inner lining.
- Heart attack.
Coronary Bypass Graft Surgery
There are several advanced, minimally invasive technologies available for treating chronic complete blockage of the coronary arteries (CTO).
The operation known as coronary artery bypass graft surgery (CABG) is performed to treat coronary artery disease. Coronary artery disease (CAD) is characterized by the narrowing of the coronary arteries, which are the blood vessels that give oxygen and nutrients to the heart muscle. CAD is caused by a build-up of fatty material inside the artery walls. This build-up narrows the arteries on the inside, reducing the delivery of oxygen-rich blood to the heart muscle.
One method of treating blocked or narrowed arteries is to replace the blocked portion of the coronary artery with a piece of a healthy blood vessel from another part of your body. Blood vessels, or grafts, utilized in the bypass procedure may be portions of your leg's vein or an artery in your chest.
An artery from your wrist may be utilised as well. Your doctor will place one end of the graft above the obstruction and the other end below it. Blood flows through the new graft to reach the heart muscle, bypassing the obstruction. This is referred to as coronary artery bypass surgery.
Traditionally, your doctor would make a major incision in your chest and temporarily stop your heart to bypass the blocked coronary artery. Your doctor will cut the breastbone (sternum) in half lengthwise and spread it apart to open the chest. Once the heart has been exposed, your doctor will implant tubes into it to allow blood to be pumped across the body via a heart-lung bypass machine. The bypass machine is required to keep blood flowing when the heart is stopped.
While the classic "open heart" procedure is still used and frequently preferable in many cases, less invasive procedures for bypassing blocked coronary arteries have been developed. Off-pump" procedures, in which the heart is not stopped, were developed in the 1990s. Other minimally invasive methods, such as keyhole surgery (done through extremely small incisions) and robotic operations (done with the assistance of a moving mechanical instrument), may be employed.
What Conditions Can CABG Surgery Treat?
Coronary heart disease, a collection of disorders that includes heart attack and coronary artery disease, is the most common cause of CABG. Angina pectoris, which is chest discomfort produced by ischemia in your heart, and silent myocardial ischemia, which is heart ischemia without any symptoms, are two more conditions classified as coronary heart disease.
Coronary heart disease is characterized by a narrowing of the arteries in your heart caused by a build-up of a fatty, wax-like residue known as plaque. As plaque accumulates on the inside of your heart's arteries, they stiffen and narrow. When an area of plaque ruptures, blood clots can develop and cause blockages in the arteries. Ischemia in parts of your heart is caused by these obstructions, which can lead to a heart attack.
What are Types of CABG Surgery?
While most individuals get CABG using the same approaches, there are times when various techniques are appropriate for your specific circumstances. Among the types of this operation are:
- Off-pump CABG. A heart-lung bypass machine is not used in this version of CABG. That is, the surgeon does not stop your heart throughout the surgery and completes all of the job while it is still beating. This form of surgery is not appropriate for every patient, and it is more difficult for the surgeon. Some surgeons, however, have particular training and expertise in doing CABG surgery in this manner.
- CABG with minimally invasive techniques. This type of CABG does not include a major incision or the splitting/lifting of your sternum and rib cage. Instead, the surgeon makes much tiny incisions and enters your heart through holes in several of your ribs. This treatment may also employ the off-pump approach.
- CABG with robot assistance. Surgical robots are advanced machines that may be used by a physician to perform CABG surgery. To do this, a surgeon "drives" the robot, controlling its motions. Robotic surgery makes smaller incisions and avoids opening and lifting your sternum. Robotic surgery may employ heart-lung bypass or the off-pump approach.
- Hybrid procedure. This method combines CABG with additional procedures or approaches. This often entails robot-assisted CABG on at least one artery, with non-CABG methods such as stenting used for the other affected blood arteries. Stenting is the insertion of a stent, a frame-like device, into an artery. Because the stent works as a skeleton inside the artery, it helps keep the artery open.
What You Need to Know Before CABG Surgery?
Preparing for CABG involves informing and educating you on what to expect and what you need to do before and after surgery to get the best possible outcome. You will learn about the following topics:
- Medications. Before the procedure, your healthcare professional will go through the drugs you're taking. They will also advise you on which drugs to continue taking and which to discontinue (and when to stop them). In some situations, they may change your prescriptions or start you on new ones.
- How to Get Ready for Surgery. Your healthcare practitioner will provide you instructions and materials to help you prepare for the surgery. This includes understanding what sort of assistance you'll require at home, what you can and cannot consume following the surgery, what essentials you'll require at home, and more. It also contains instructions on how to bathe (typically with special soap) and groom oneself before to the surgery.
- What to Expect Following Surgery. Your healthcare practitioner will also offer you with information and tools outlining what to expect during your recuperation. This covers how long it will take you to heal, how you will feel, signs to look out for, and other information.
Advantages of CABG Procedure
CABG offers various features that make it a valuable and popular treatment option for cardiac issues.
- A long history of usage. In the early 1960s, surgeons conducted the first CABG surgeries. Additional studies and advancements in the decades thereafter have contributed to make this method a vital and dependable approach for treating cardiac ischemia.
- Better for many blockages or specific artery blockages. When a person has numerous blocked arteries in their heart, CABG is frequently the best option. It's also a better method for removing obstructions in specific areas. Many studies have linked CABG to better long-term results, including a higher chance of survival. This advantage typically rises when combined with modern bypass procedures that produce long-term outcomes.
- Reduced risk for follow-up procedures. Percutaneous coronary intervention (PCI), often known as angioplasty, is the primary alternative to CABG. PCI has a greater probability of requiring a follow-up operation in many circumstances.
Percutaneous Coronary Intervention (PCI)
A percutaneous coronary intervention (PCI) is a minimally invasive treatment used to unblock clogged coronary arteries in the heart. Coronary angioplasty with stenting, or angioplasty for short, is an older term for PCI.
Arteries are blood vessels that transport oxygen-rich blood from your heart to the rest of your body. A PCI technique employs a tiny balloon to unblock a blocked artery and enhance blood flow.
Your interventional cardiologist will next insert a small, permanent tube (stent) to keep the artery open permanently. To reduce the risk of re-narrowing within the stent, the stent often contains medication that is released directly into your artery (drug-eluting stent).
Who Needs PCI?
A PCI procedure may be required to remove build-ups of a thick, fatty material called plaque from your arteries. Atherosclerosis is caused by plaque that accumulates and hardens in your arteries.
Atherosclerosis raises the risk of cardiovascular disease and restricts blood flow to the heart. Your heart is not pumping blood efficiently, and you may have chest discomfort (angina).
PCI may potentially be used as a heart attack therapy by healthcare practitioners. PCI opens blood arteries fast, which can help reduce heart damage.
Who shouldn't have a PCI?
You and your doctor will decide which treatment is best for you.
Whether you have PCI, medical treatment, or coronary artery bypass graft (CABG) surgery is determined by a number of factors, including:
- The number and characteristics of the blockages that you have.
- Other cardiac and non-cardiac medical conditions.
- Your heart muscle function and age.
What Happens During PCI?
The PCI is performed by an interventional cardiologist (a clinician who specializes in the heart, blood vessels, and circulatory system). You are given a sedative (anesthesia) to help you remain quiet and comfortable during the procedure. You are normally conscious but have no sensation during the process.
During a PCI, a cardiologist will:
- Insert a short hollow tube (sheath) into a blood vessel in your arm or leg.
- A tiny, hollow tube (catheter) is guided through the sheath and into your heart.
- Injects a contrast dye into the catheter and utilizes X-rays to observe it in real time.
- By inflating a balloon at the catheter's tip, the blocked artery is opened.
- A stent is inserted if necessary to maintain the artery open.
- The catheter is removed, and the insertion site is closed with a compression bandage (arm), a tiny stitch (thigh), or a collagen plug (thigh).
The treatment normally takes between 30 minutes and two hours to complete. The exact treatment period is determined by a number of factors, including the degree of plaque build-up.
High Risk Percutaneous Coronary Intervention (CHIP)
A rising number of patients with coronary artery disease (CAD) require stent PCI or coronary artery bypass graft surgery but have been told they are too high-risk for problems during these operations. These patients are dealing with increasing chest pain, shortness of breath, tiredness, and heart failure since they have no therapy alternatives.
To address this growing population of high-risk CAD patients, North-western Memorial Hospital interventional cardiologists have demonstrated excellent clinical outcomes using an advanced catheter-based procedure called Complete Higher Risk Indicated Percutaneous Coronary Intervention (PCI) or CHIP to open blocked coronary arteries in the high-risk patient.
A number of factors may lead to a patient being considered high-risk and a candidate for CHIP including:
- Advanced age.
- History of disease including kidney disease, stroke or diabetes.
- Location of CAD including left main or bifurcated disease.
- Challenging plague types including calcified or long lesions.
- Coronary artery chronic total occlusion (CTO).
- Previous open heart surgery.
- Heart failure.
Are Complex Coronary Interventions Too Risky?
Because complicated coronary procedures are significant operations, there are considerable risks and complications. While the majority of these risks and problems are preventable or treatable, it is still critical to be aware of them. Risks include:
- Heart rhythm irregularities (arrhythmias). Atrial fibrillation, which increases the risk of stroke, is the most prevalent arrhythmia after major coronary procedures. Fortunately, it is typically only a short-term issue.
- Bleeding. This is a possibility with any major operation. To avoid this, patients who use blood thinners must discontinue them (under the supervision and direction of their healthcare professional) before to surgery.
- Infections. Infection is another possible surgical consequence. When infections spread throughout your body, they can induce sepsis, a potentially fatal immune system response. Sepsis is a medical emergency, and having two or more of its symptoms (rapid heart rate, fever, chills, disorientation, rapid breathing, or confusion) is as deadly as having a heart attack or stroke. Fortunately, due to better surgical care and methods, severe infections following CABG are uncommon.
- Delirium or confusion. These induce symptoms such as anxiousness, difficulty thinking clearly, memory issues, or unusual behaviour (where they seem like a different person).
- Kidney problems
- Stroke.
- Heart attack.
Conclusion
In the United States, coronary artery disease is the leading cause of mortality for both men and women. If not treated appropriately, a blockage in the heart arteries can induce a heart attack and eventually lead to heart failure. The most common symptoms of coronary heart disease (CHD) are chest pain (angina) and breathlessness. But some people may not have any symptoms before they're diagnosed.
Patients with severe or complex coronary artery disease can be treated by a cardiologist. If you have previously had unsuccessful angioplasty or stenting procedures, if you have been told there are no options to fix your coronary blockages, if you have been told you are at high risk for open heart bypass surgery, or if you continue to experience severe symptoms despite having tried all standard treatments, you may have complex coronary disease.
Interventional cardiologists are experts at performing minimally invasive procedures to repair difficult-to-treat blockages as well as safely performing operations on patients who have medical issues that increase procedure risk.
Many cardiologists have extensive expertise employing cutting-edge equipment and procedures to treat patients with severe calcification (atherectomy), side branch blockages (bifurcation stenting), complete coronary artery occlusion (CTO), and patients at high risk owing to poor heart function (mechanical circulatory support).