Device Closure of Atrial Septal Defect (ASD)
Overview
A common congenital cardiac problem, atrial septal defect (ASD), has a reported frequency of 1.0/1000 live births. Untreated ASD can lead to right ventricular overload and right heart failure, as well as atrial arrhythmias, systemic embolism, pulmonary hypertension, and mortality. Transcatheter closure of isolated secundum ASD has become the recommended therapeutic method in the majority of instances during the last 15 years. This technique has shown significant evidence of positive long-term effects at high-volume institutions.
ASD Secundum closure using transcatheter device is a mature technology that has been around for more than a decade. This therapy has become a widely acknowledged alternative to surgical therapy, and it is usually viewed as safe and successful.
What is Atrial septal defects (ASD)?
Atrial septal defects (ASD) are divided into four types: ostium primum, ostium secundum, sinus venosus, and coronary sinus. ASD is currently estimated to account for 10% of congenital heart abnormalities. Although ASD is characterized as a generally benign form of heart illness, natural history studies show that if left untreated, it can eventually contribute to severe morbidity and mortality.
Untreated ASD can result in right ventricular volume overflow, right heart failure, increased pulmonary vascular resistance, systemic embolism, and atrial arrhythmias. Only the ostium secundum defect among the many forms of ASDs is amenable to device closure, but all four varieties can be surgically closed. Routine closure of ASD in children has been justified throughout the years due to the availability of low-risk, curative surgical and transcatheter treatments.
Atrial septal defects Symptoms
Asymptomatic atrial septal abnormalities are common. A quiet, systolic ejection murmur across the pulmonic region (second intercostal space) is accompanied with a broad, fixed splitting of S2. Many ASDs go misdiagnosed until adulthood, therefore treatment, particularly for significant deficits, is frequently delayed. Large abnormalities that go untreated can lead to exercise intolerance, cardiac dysrhythmias, palpitations, an increased risk of pneumonia, pulmonary hypertension, and death.
Eisenmenger syndrome is an uncommon yet severe consequence of untreated ASDs induced by continuous overflow vascular remodeling (through a left-to-right shunt). Right atrial pressures approach systemic as vascular resistance rises. When right atrial pressures reach systemic pressures, shunt flow reverses. Patients with Eisenmenger syndrome suffer persistent cyanosis, increased pulmonary vascular resistance, exertional dyspnea, syncope, and an increased susceptibility to infection.
People with minor heart abnormalities (less than 5 mm) may not experience any symptoms, but patients with defects ranging from 5 to 10 mm will experience symptoms in their fourth or fifth decade of life. Patients with greater abnormalities present earlier, in their third decade. Patients may complain of dyspnea, weariness, inability to exercise, palpitations, or indications of right-sided heart failure. Preoperatively, around 20% of adult patients develop atrial tachydysrhythmias. Evidence of a stroke or transient ischemic event, particularly after the diagnosis of a peripheral blood clot, should raise concerns for an ASD.
How is Atrial septal defect diagnosed?
Diagnostic imaging is critical in establishing the magnitude of the lesion as well as treatment alternatives. The gold standard imaging modality is a transthoracic echocardiography. A transthoracic echocardiogram can detect the size of the defect, determine the direction of blood flow, identify associated abnormalities (involvement of endocardial cushions and atrial-ventricular valves), examine the heart for structure and function, estimate pulmonary artery pressure, and calculate the pulmonary/systemic flow ratio (Qp/Qs). A transesophageal echocardiography is a more accurate method for detecting uncommon heart abnormalities.
Although echocardiography is the gold standard for evaluating ASDs, cardiac CT and MRI are also diagnostic modalities. CT and MRI both look at structures around the heart and in the thoracic cavity. Although chest x-ray results are not as diagnostically useful, they do help clinicians monitor clinical condition by recognizing cardiomegaly and pulmonary artery enlargement.
Exercise testing can aid in determining the reversibility of shunt flow and the responsiveness of pulmonary artery hypertension patients to activity. Cardiac catheterization is not recommended in individuals who are young and have small, uncomplicated ASDs.
Atrial septal defects Management
In the first year of life, patients with atrial septal defects smaller than 5 mm in size typically have spontaneous closure of the defect. Defects larger than 1cm in length will almost certainly need medical/surgical intervention to close. Control of the aberrant rhythm and anticoagulation are required for patients who come with atrial dysrhythmias; final intervention can occur once the team has gained control of the dysrhythmia.
Adult patients with minor abnormalities and no symptoms of right heart failure should be monitored. Every 2 to 3 years, an echocardiogram is performed to assess the function and anatomy of the right heart. A history of TIA or stroke necessitates more extensive surveillance and, in certain cases, surgical intervention.
Percutaneous and surgical intervention are alternatives for ASD closure. Stroke, a hemodynamically significant shunt bigger than 1.5:1, and signs of systemic oxygen desaturation are all indications for therapy. Percutaneous transcatheter closure is less risky for the patient, however it is only beneficial for ostium secundum defect closure. Percutaneous transcatheter ASD closure had a 7.2% post-procedural complication risk against a 24% post-surgical complication risk.
Spontaneous ASD closure in the first year of life is prevalent in patients with ASD less than 5mm. Medical or surgical closure is frequently required for defects bigger than 1cm. Previously, surgical closure was the standard of therapy for ASD, but transcatheter devices have quickly established as the norm in children during the last 40 years.
Widespread device usage and rather lax post-market surveillance revealed device degradation leading in cardiac perforation, a previously unknown and possibly catastrophic adverse event. The crucial U.S. Food and Drug Administration (FDA) device trials found no evidence of erosion. The FDA convened a group to assess the authorized ASD closure devices after receiving several reports of erosions.
What is atrial septal defect transcatheter repair for children?
Transcatheter atrial septal defect (ASD) repair is a treatment used to repair a hole in the atrial septum. The atrial septum is a wall that divides the heart's right and left upper chambers (atria). This gap is known as an atrial septal defect, or ASD.
Blood can flow irregularly from the left atrium into the right atrium if this abnormality exists. This leads the heart to send more blood to the lungs. If left untreated for an extended period of time, this additional blood might cause damage to the lung blood vessels. In addition, the right-side pumping chamber (right ventricle) might grow. As a result, it needs to work more than usual to push blood to the lungs.
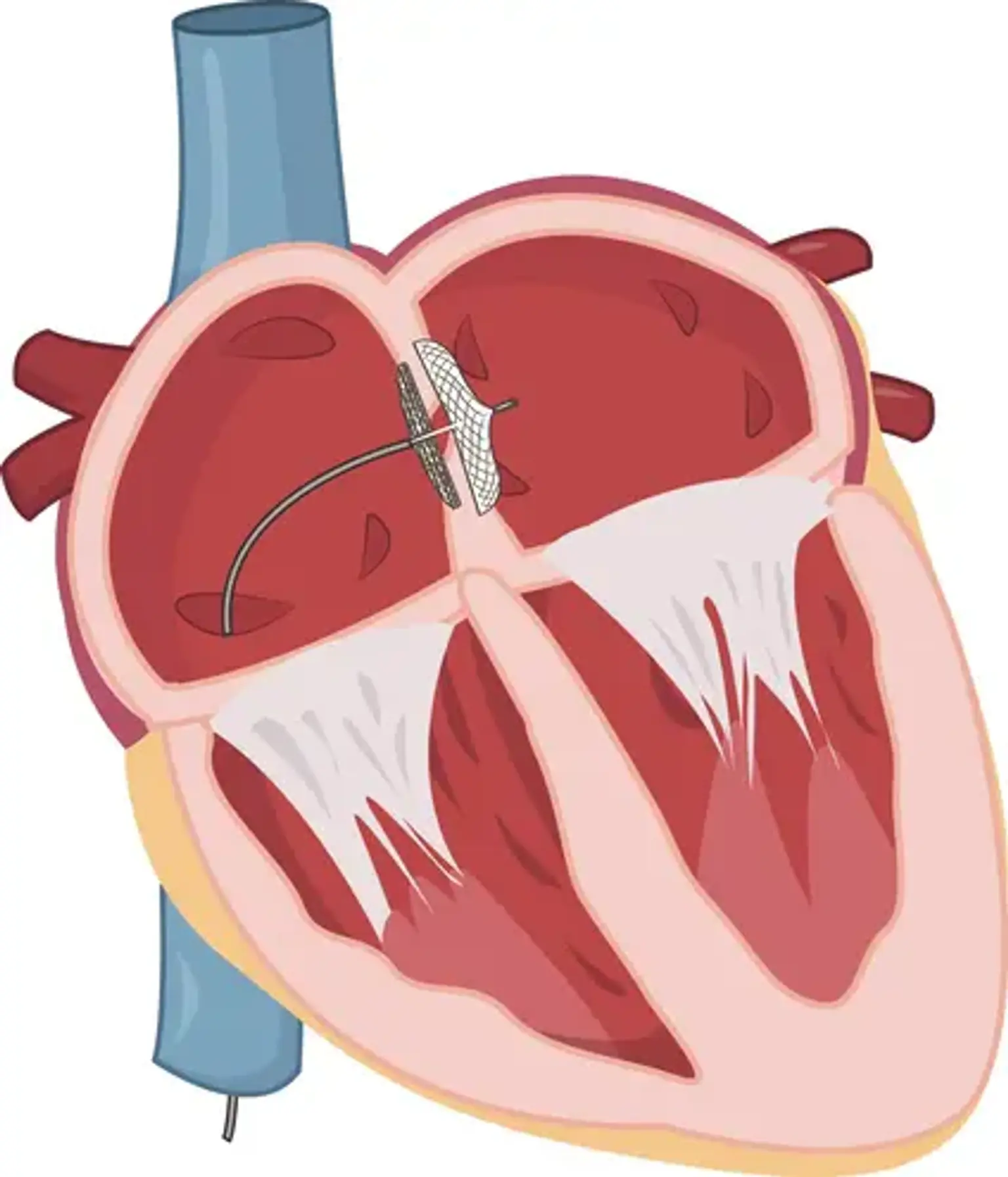
To seal this hole, ASD transcatheter repair employs a long, flexible tube (a catheter) and a tiny device. The catheter is inserted into a blood vessel in the groin by an interventional cardiologist. A little gadget folded up like an umbrella is contained within the catheter. The catheter is advanced all the way to the heart's septum by the cardiologist. The tiny device emerges from the tube and seals the opening in the atrial septum. The catheter is then removed from the body by the cardiologist. Tissue develops over the device over time, securing it even more securely.
The advantages of transcatheter device closure are:
- There is no requirement for cardiopulmonary bypass (heart-lung machine use) or cardioplegia (temporarily stopping the heart).
- There is no visible surgical scar on the chest. After the treatment, there are simply minor needle puncture scars in the groin area; sutures are not required.
- In comparison to surgery, there is very little discomfort.
- Shorter hospital stay – the youngster can be discharged the same day.
Not all atrial septal defects are acceptable for transcatheter device closure, and patients must be thoroughly evaluated before this type of closure is recommended. There are many devices available for transcatheter ASD closure.
Why might your child need an atrial septal defect transcatheter repair?
At birth, every infant has a typical little opening between the left and right atria. This hole frequently closes or shrinks shortly after delivery. However, it remains open in some children. Most doctors have no idea why this occurs.
Many children with ASD may not require the hole to be fixed. Smaller holes may not allow much blood to travel between the atria. The heart and lungs do not have to work any harder than usual in these situations. These tiny holes do not produce symptoms and do not require repair. These little holes will sometimes shut on their own. A healthcare physician may decide to wait and see if that occurs before doing a repair, especially in a very young kid.
If your child has a more severe ASD, he or she may require some form of repair. Children with more severe ASDs may have symptoms such as shortness of breath. A big, unrepaired ASD might potentially produce elevated blood pressure in the lungs' arteries. This, in turn, might result in low oxygen levels in the body. Even if the youngster does not yet exhibit symptoms, healthcare practitioners frequently propose a repair. It has the potential to prevent long-term, chronic lung damage. The operation is most commonly performed on youngsters. However, if their ASD was not discovered during infancy, adults may require this sort of correction.
ASD transcatheter repair is less invasive than surgical repair. It also takes less time to recuperate. Transcatheter repair is frequently used instead of surgery when it is a possibility. Transcatheter repair is only achievable for specific types of ASDs, such as those in the septum's center (referred to as "secundum"). Other portions of the septum with atrial abnormalities require surgical correction. Large ASDs may also necessitate surgical correction. Transcatheter repair may also be ruled out if a kid has other cardiac abnormalities that require treatment at the same time.
What happens during an atrial septal defect transcatheter repair for a child?
Discuss what to expect throughout the procedure with your child's healthcare professional. Generally speaking:
- Your child will get anesthesia before the surgery starts. Your child will sleep deeply and painlessly during the procedure. He or she won’t remember it afterward.
- The repair will take about 2 hours.
- The healthcare provider will insert a small, flexible tube (catheter) into an artery in the groin. This tube will have a small device inside it.
- The tube will be threaded into the blood vessel all the way to the atrial septum by the healthcare professional. To determine the exact location of the tube, X-ray pictures and an echocardiography may be employed.
- In some situations, the healthcare professional may utilize a transesophageal echocardiography, which involves inserting an ultrasound probe into the child's throat.
- The little device will be pushed out of the tube and placed across the opening in the atrial septum by the healthcare provider. The gadget will then be secured in place.
- The tube will be removed through the blood vessel.
- The healthcare provider will close and bandage the site where the tube was inserted.
What happens after an atrial septal defect transcatheter repair for a child?
Ask your child’s healthcare provider what will happen after the ASD transcatheter repair. You can generally expect the following:
- Your youngster will be in a recovery room for many hours.
- The vital indicators of your child, such as heart rate and respiration, will be monitored.
- After the treatment, your kid may need to lie flat for several hours without bending his or her legs. This will aid in the prevention of bleeding.
- Your child's doctor may prescribe medication to keep his or her blood from clotting (anticoagulants).
- If pain medication is required, your kid will receive it.
- Your child's doctor may recommend further testing, such as an electrocardiogram or an echocardiography.
- Your child will most likely need to spend at least one day in the hospital.
At home after the procedure:
- Inquire about the medications your child need. Your kid may need to take antibiotics or drugs to prevent blood clots for a short period of time. As required, provide pain relievers.
- Avoid intense activity with your youngster. Encourage him or her to take a break.
- Any sutures will be removed at a later date. Keep track of all follow-up appointments.
- If your kid has increasing edema, excessive blood or drainage, a fever, or severe symptoms, contact a healthcare practitioner. A small amount of drainage from the location is typical.
- Follow all medication, exercise, food, and wound care advice given to you by your child's healthcare practitioner.
Your child will require regular monitoring by a cardiologist for a short period of time following the surgery. After that, your child will only need to see a cardiologist on an as-needed basis. Your kid may require antibiotics before some medical and dental treatments for a while after the surgery to help avoid an infection of the heart valves.
What are the risks of atrial septal defect transcatheter repair for a child?
The majority of youngsters respond favorably to ASD transcatheter correction. However, difficulties can occur on occasion. Overall, the risk of complications is lower than with surgery. Age, the magnitude of the abnormality, and other health issues can all be risk factors. Possible hazards include:
- Abnormal heart rhythms
- Device becoming unattached and moving through the heart or vessels (embolization)
- Buildup of fluid around the heart
- Infection
- Excess bleeding
- Puncturing the heart (rare)
- Tear in the groin blood vessel where the catheter is inserted
- Temporarily reduced blood flow to the heart
- Collection of blood (hematoma) in the groin
It is also conceivable that the operation will fail to cure the ASD. Inquire with your kid's doctor about the unique risk factors for your child.
Conclusion
One of the most prevalent congenital heart disorders (CHDs) and the most frequent CHD in adults is atrial septal defect (ASD). Transcatheter closure of ostium secundum atrial septal defects has become a viable alternative to surgical correction (ASD). Large ASDs (>38 mm) and defects with insufficient rims, on the other hand, are typically not provided transcatheter closure and are sent for surgical closure.