Ventriculoperitoneal (VP) Shunt Surgery
Overview
Hydrocephalus is a disorder defined by an abnormal buildup of cerebrospinal fluid (CSF) in and around the brain, causing swelling and impairing normal brain function. The surgical installation of a medical device known as a shunt is the most frequent therapy for hydrocephalus.
What is a Ventriculoperitoneal Shunt?
A ventriculoperitoneal (VP) shunt is a cerebral shunt that drains excess cerebrospinal fluid (CSF) when the usual outflow is obstructed or there is a reduction in fluid absorption. Hydrocephalus is treated by cerebral shunts. Untreated hydrocephalus in children can cause a variety of side effects, including increased irritability, persistent headaches, learning difficulties, vision impairments, and, in extreme cases, severe mental retardation.
If it fails after implantation, extra CSF accumulates, increasing intracranial pressure, resulting in cerebral edema and, eventually, herniation. These shunts drain CSF into the peritoneum, atrium, or pleura, and are so correctly referred to as ventriculoperitoneal, ventriculoatrial, and ventriculopleural shunts.
A shunt is made up of a ventricular catheter attached to a valve and subsequently to a distal catheter. A VP shunt's distal end is inserted into the peritoneal cavity. The key distinctions between shunts are the type of valve utilized and whether or not the valve is programmable. Biotechnology advancements are causing gradual alterations in the shunt components. These cutting-edge components are intended to minimize shunt failures and improve neurosurgery patient care.
Anatomy and Physiology
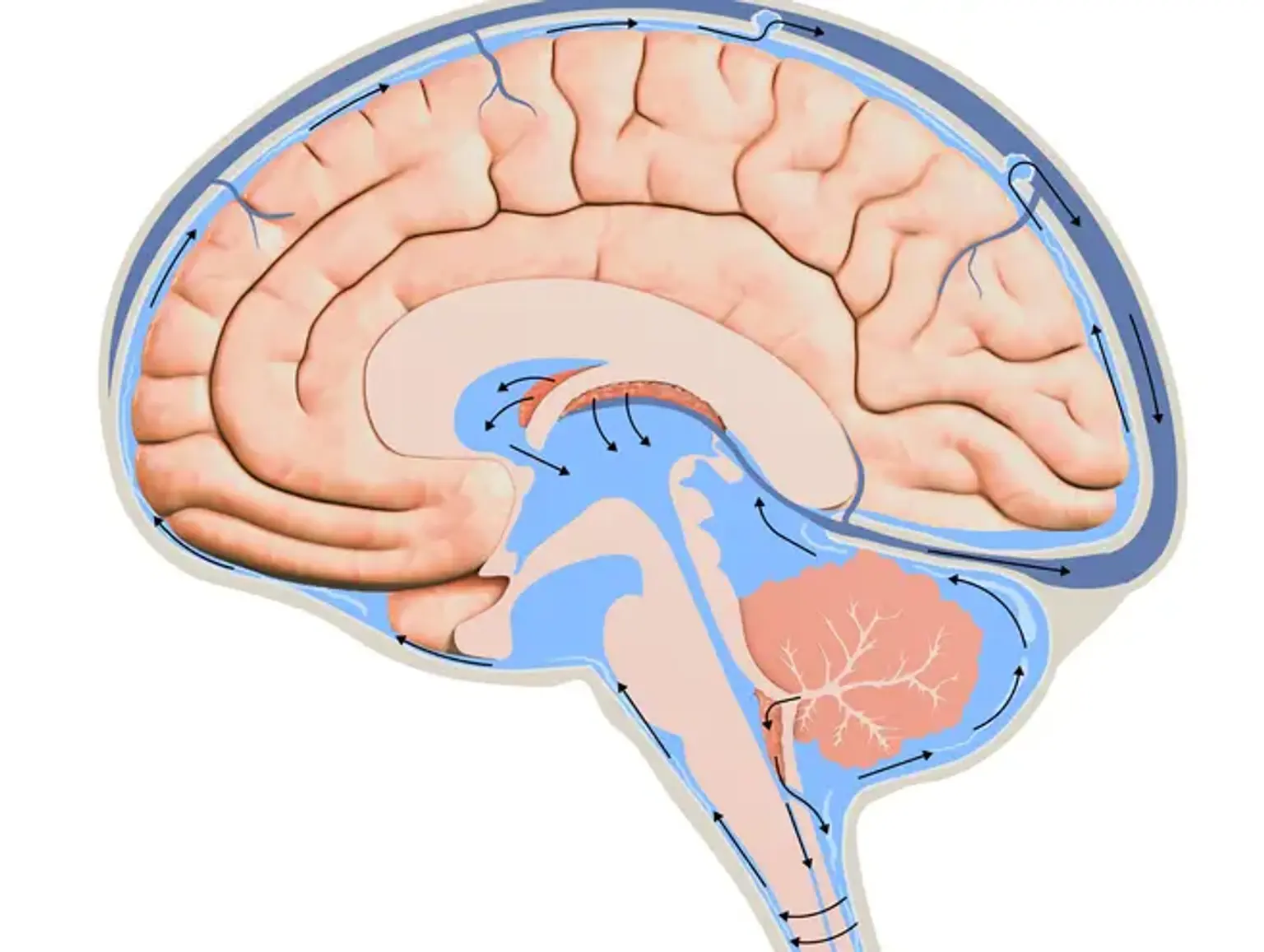
The ventricles of the brain are a network of chambers that communicate inside the brain parenchyma. Two lateral ventricles, the third ventricle, the cerebral aqueduct, and the fourth ventricle comprise the ventricular system. CSF is produced by the choroid plexus in the ventricles and fills the ventricle and subarachnoid space in a continual cycle of production and reabsorption.
The Pacchionian (arachnoid)granulations then absorb the CSF into the cerebral venous circulation. Any blockage or restriction in this channel will result in obstructive hydrocephalus, which, if persistent, will need the use of a shunt. These granulations can get clogged by blood products or excessive protein levels and fail to function properly, resulting in communicating hydrocephalus.
The surgeon's preference governs the placement of a cerebral shunt and its location. It can be inserted into the lateral ventricles by a frontal approach or a parieto-occipital approach into the trigone or occipital horn. The catheter that is inserted into the cerebral ventricle is referred to as the proximal shunt (ventricular catheter), suggesting its close proximity to the brain.
The right lateral ventricle is the most preferable location for a proximal shunt since any complications will not be connected with the dominant hemisphere. If asymmetry exists, the bigger ventricle is used. If all prior sites have been exhausted, the distal catheter can be inserted in the belly (peritoneal cavity), heart through a cervical venous access, chest cavity (pleura), or, in rare cases, the ureter or bladder. However, in all circumstances, the distal end of the catheter can be placed in any tissue that has cells capable of absorbing the entering CSF.
A subgaleal shunt is a temporary remedy used in newborns who are too little or preterm to tolerate conventional shunts or who have peritoneal absorption difficulties. The surgeon creates a pocket beneath the subgaleal area and allows CSF from the ventricles to drain, resulting in a fluid-filled bulge on the infant's head. These shunts are subsequently changed to permanent shunts as the youngster develops.
Indications for VP Shunts
The majority of VP shunts are used to treat hydrocephalus. The following are examples of disorders that frequently necessitate shunting:
- Congenital hydrocephalus following aqueductal stenosis is a hereditary condition that causes nervous system deformations and is linked to mental retardation, abducted thumbs, and spastic paraplegia.
- Tumors that cause CSF blockage in the lateral ventricles, third ventricle, and posterior fossa, as well as those that obstruct the cerebral aqueduct or fourth ventricle
- Communicating hydrocephalus secondary to meningitis or subarachnoid hemorrhage
- Hydrocephalus develops as a result of myelomeningocele because the flow of CSF is changed owing to hindbrain abnormality.
- Craniosynostosis occurs when the sutures of the skull shut prematurely, resulting in sutures fusing before the brain stops developing and, in rare cases, hydrocephalus.
- Dandy-Walker syndrome is distinguished by a fourth ventricle cystic malformation, hypoplasia of the cerebellar vermis, and an expanded posterior fossa.
- Arachnoid cysts are a defect that occurs when CSF collects and becomes caught in the arachnoid membranes, resulting in a blockage of the normal flow of CSF and hydrocephalus.
- Idiopathic intracranial hypertension is a rare neurological illness that affects around one in 100,000 persons, mostly women of reproductive age, and causes an increase in intracranial pressure, which can result in irreversible eyesight loss.
- Normal-pressure hydrocephalus resulted in the usual trio of memory/dementia difficulties, gait impairment, and urine incontinence.
What are the most common Shunt Systems?
The most common shunt systems are:
- Ventriculoperitoneal (VP) shunts. This form of shunt redirects CSF from the brain's ventricles to the peritoneal cavity, which houses the digestive organs in the belly. The distal catheter tip lies in this hollow close but not inside the gut and bowel loops. This CSF is reabsorbed into the circulation and subsequently expelled through regular urine.
- Ventriculoatrial (VA) shunts. This form of shunt redirects CSF from the brain's ventricles to the right atrium of the heart. The distal catheter is inserted into a vein in the neck and carefully moved into the right atrium of the heart. The CSF enters the circulation immediately and is then expelled through regular urine.
- Ventriculopleural (VPL) shunts. This form of shunt redirects CSF from the brain's ventricles into the pleural (chest) cavity. This gap exists between the chest wall and the lungs. It is bordered by pleural fluid and a membrane that runs along the chest wall (parietal pleura membrane) and the lung surface (visceral pleura membrane). The CSF is mixed with this fluid and is absorbed and expelled normally by urine.
- Lumboperitoneal (LP) shunts. This is a one-of-a-kind shunt that diverts CSF from the intrathecal space within the spine rather than the brain (rather than commencing in the brain). The CSF is sent into the peritoneum. This CSF is reabsorbed into the circulation and subsequently expelled through regular urine. See the VP shunt description above for more information on the peritoneal cavity.
Preparation for Ventriculoperitoneal Shunt Placement
Preoperative preparation for ventriculoperitoneal shunt placement generally involves the following steps:
- A thorough examination is performed by your doctor to check for any medical issues that need to be addressed prior to surgery.
- Depending on your medical history, social history, and age, you may need to undergo blood work and imaging tests to help detect any abnormalities that could compromise the safety of the procedure.
- You will be asked if you have allergies to medications, anesthesia, or latex.
- You should inform your doctor of any medications, vitamins, or supplements you are taking.
- You may need to stop taking vitamin supplements such as Vitamin E, herbal remedies, or medications such as blood-thinners or anti-inflammatories a week or two prior to surgery.
- You should refrain from alcohol or tobacco at least a week before surgery.
- You should not consume any solids or liquids at least 8 hours prior to surgery.
- Arrange for someone to drive you home after surgery.
- A written consent will be obtained from you after the surgical procedure has been explained in detail.
What Can I Expect During the VP Shunting Procedure?
VP-shunt placement normally takes 90 minutes while the patient is under general anesthesia. A little patch of hair is shaved off the head (typically at the top) or behind an ear to prepare the region for an incision. To get access to the brain, a U-shaped incision is made and a hole is formed in the overlying skull. A catheter is then inserted into a brain ventricle, frequently with the surgeon utilizing an endoscope or a computer-guidance system to acquire a good picture of the region.
A second catheter is put beneath the skin near the back of the skull and threaded down until it reaches the abdomen's peritoneal cavity. In order to appropriately situate the catheter, an incision is made in the abdomen. A very small pump is also implanted at the location of the incision on the skull, and it is connected to each of the catheters. As fluid levels around the brain rise, the pump starts, safely emptying the required volume of CSF into the belly.
Many of the pumps used in VP-shunt surgery feature variable-pressure valves, which allow the flow of CSF out of the brain to be controlled, resulting in more efficient hydrocephalus therapy. There are various variable-pressure valves available; the surgeon selects one is most suited based on the patient's condition prior to the treatment.
VP Shunting Recovery
This section will inform you of what to expect following your operation. You will learn how to recuperate safely following surgery both in the hospital and at home. Make a list of questions to ask your healthcare professional as you go through this section.
Pain medication
Medication will be used to treat your pain while you are in the hospital. A staff member will escort you to your hospital room once you have recovered from the anaesthetic. The length of your stay in the PACU may also be determined by when your hospital bed becomes available.
The amount of time you spend in the hospital following surgery is determined by your recuperation. The average hospital stay is one to two days. When you are transported to your hospital room, you will meet one of the nurses who will be caring for you while you are there. Your nurses will educate you how to care for yourself while you are in the hospital recovering from surgery.
Your nurses will do basic tests to ensure that your brain is functioning properly in the days after your operation. They'll do stuff like:
- Ask you questions such as where you are and what time of day it is.
- Ask you to move your arms and legs.
- Shine a small light into your eyes to check the response of your pupils.
Moving Around and Walking
Walking and moving around will help minimize your risk of blood clots and pneumonia (lung infection). It will also assist you in resuming bowel motions and passing gas. If necessary, your nurse, physical therapist, or occupational therapist will assist you in moving around.
Exercising Your Lungs
It is critical to exercise your lungs so that they can fully expand. This helps to avoid pneumonia.
- Use your incentive spirometer 10 times every hour you’re awake.
- Do coughing and deep breathing exercises. A member of your care team will teach you how.
Eating and drinking
Following your procedure, you will be given ice chips to consume. You'll start with a liquid diet and then gradually resume eating your typical meals as tolerated. If you have any concerns about your diet, make an appointment with a professional dietitian nutritionist.
Imaging scan
You may get a computed tomography (CT) scan of your head 1 to 2 days following surgery to ensure the shunt is in the proper location. Before the scan, your nurse will provide you with further information.
Caring for your incision
Your incision will be wrapped in bandages. They will be removed by your doctor one to two days following your procedure. You can then leave them exposed. For the first 5 days following surgery, avoid getting your incision wet or applying lotions, creams, or powders to it.
Planning for your discharge
A physical therapist will work with you before you leave the hospital to determine if you require home care assistance, such as special medical equipment or a home care nurse. After you are discharged from the hospital, your case manager will work with you to arrange for home care visits if necessary.
While you heal at home following surgery, a caregiver should assist you. Your incision will have begun to heal by the time you are ready to leave the hospital. Examine your incision with your nurse before leaving the hospital. Knowing the appearance of your incision will help you spot any changes later.
If your transport isn't at the hospital when you arrive, you might be permitted to wait in the Patient Transition Lounge. More information will be provided by a member of your healthcare team.
Call your healthcare provider if:
- The skin around your incisions is very red.
- The skin around your incisions is getting more red.
- You see drainage that looks like pus (thick and milky).
If you go home with staples or stitches in your incisions, your doctor will remove them during your first post-surgery checkup. This normally happens 7 to 10 days following your procedure.
Showering
- Shower for five days following your procedure. During this time, you may take a sponge bath, but avoid getting your incision wet. Use dry shampoo, creams, or lotions away from your incisions.
- Take a shower every day for the next 5 days to clean your incision. It's fine to get your staples wet if they're in your incision.
- During your shower, use gentle shampoo, such as baby shampoo, and soap. After showering, wipe dry the area with a clean towel and leave your incision exposed. Apply no creams, lotions, or powders on your incision.
Physical activity and exercise
When you leave the hospital, your incision will appear to be healed on the exterior but not on the inside. During the first 4 to 6 weeks following your surgery:
- Don’t lift anything heavier than 10 pounds (about 4.5 kilograms).
- Don’t do any strenuous activities (such as jogging and tennis).
- Don’t play any contact sports (such as football).
Aerobic activity, such as walking and stair climbing, will help you acquire strength and improve your mood. Walk for 20 to 30 minutes at least twice a day. You may go for a walk outside or within your neighborhood mall or retail center.
It is common to feel less energetic following surgery. Each person's recovery period is unique. Increase your daily activities as much as possible. Always alternate between times of activity and relaxation. Rest is an essential component of your rehabilitation.
Driving
Consult your doctor about when you will be able to drive. Most people can resume driving four to six weeks following surgery. Do not drive if you are taking pain medication that may cause drowsiness. After you leave the hospital, you can travel in a car as a passenger at any time.
Going Back to Work
Discuss your job with your healthcare practitioner. Based on what you do, they'll inform you when it's safe for you to return to work. You may need to remain out a bit longer if you move around a lot or lift large stuff. You may be able to return sooner if you sit at a desk.
Traveling
You have the option of traveling by bus, rail, or vehicle. Do not fly until your doctor gives you the all-clear. When traveling a long distance, avoid sitting for extended periods of time. Every 2 hours, take a break and go about. This will aid in the prevention of blood clots in your legs.
Ventriculoperitoneal Shunting Possible Risks
Although VP shunting is a highly safe treatment, there are some uncommon but substantial dangers. Excessive bleeding, infection, and adverse responses to anesthesia, such as breathing difficulties, changes in heart rate, or changes in blood pressure levels, are risks connected with every surgical treatment. Other dangers associated with a VP shunt include:
- Infection in the shunt or brain
- Blood clots
- Bleeding in the brain
- Damage to brain tissue
- Swelling of the brain
- Abdominal pain
If you develop any of these symptoms, or symptoms that the VP shunting treatment was meant to cure, such as headaches, seizures, or lack of coordination, it might be a sign of an infection or a shunt malfunction, and you should contact your doctor right once.
Conclusion
Ventriculoperitoneal (VP) shunting is a neurosurgery technique intended to reduce brain pressure caused by excess fluid accumulation. It is primarily used to treat hydrocephalus, a disease in which cerebrospinal fluid accumulates in the ventricles of the brain. This places strain on the brain, which can result in neurologic symptoms or even brain damage. Infants and the elderly are the most vulnerable to hydrocephalus.